
5.1 Responding to Inquiries from the Media
The Administration for Children and Families (ACF) Office of Refugee Resettlement (ORR), committed to both public transparency and the well-being of unaccompanied children (UC), has established clear policies for responding to media inquiries. These policies ensure that ORR and its funded care providers prioritize the best interests of UCs while maintaining accountability to the public. This programmed care approach emphasizes a case-by-case evaluation of each media request, balancing transparency with the critical need to protect the privacy and safety of children under our care.
Media personnel may approach ORR-funded care providers seeking background information, interviews with staff or UCs, or facility tours. Grantees are authorized to address a wide range of media inquiries concerning their organization’s operations, as detailed in Section 5.1.1 Policies for ORR Grantees. For media requests exceeding the scope of care provider responsibilities, as outlined in Section 5.1.2 How ORR Responds to Press Inquiries, ORR collaborates with ACF and/or the U.S. Department of Health and Human Services (HHS) to formulate appropriate responses.
Revised 08/01/2024
5.1.1 Policies for ORR Grantees
When addressing media inquiries, grantees must adhere to the following guidelines, ensuring programmed care standards are upheld in media relations:
- Care provider organizations can discuss their own organizational activities but should not comment on the activities of other grantees. For inquiries regarding ORR, its programs, or federal policy related to UCs, reporters should be directed to the ACF Office of Public Affairs at 202-401-9215.
- To safeguard the privacy and security of children in care, neither ORR nor its grantees will discuss specific cases or individual UCs with the media or public.
- The addresses of shelters must remain confidential and not be publicized. If a reporter obtains a shelter address through other channels, the organization should explain the security reasons for non-disclosure. Media access to shelters and facility tours or visits are prohibited without ORR authorization. Requests for facility tours will be managed by ORR as described in Section 1.4 Requests to Visit a Facility, prioritizing UC security, privacy, and minimal program disruption.
In addition to these mandatory policies, ORR recommends that care providers adopt media relations “best practices.” These include: developing key talking points to facilitate clear and effective communication with the media; directing media outlets to the ORR website and other resources for comprehensive information about ORR’s UC Bureau; and preparing staff handling press inquiries to effectively address common questions and highlight the organization’s accomplishments and contributions. Facilities experiencing a high volume of inquiries or facing complex requests should seek guidance from ORR.
Revised 08/01/2024
5.1.2 How ORR Responds to Press Inquiries
ORR care providers may receive media inquiries beyond their expertise or authority, or that do not align with the standards outlined above. These may include questions about ORR policies, national program activities, requests to interview specific UCs, and data requests concerning UC numbers, demographics, or program details. In such instances, care providers must immediately forward these requests to their ORR/Project Officer (PO), copying the ORR/Federal Field Specialist (FFS) and ORR communications staff. ORR, working with ACF and/or HHS, will then provide an official, accurate, and current response to the media. During influx events, ACF/ORR may implement specific procedures to manage high volumes of inquiries efficiently.
Revised 08/01/2024
5.1.3 Requests to Interview a Specific Child
Protecting the privacy and well-being of UCs is paramount. Therefore, ORR policy generally prohibits media interviews with children in ORR care. However, in exceptional situations, ORR may consider interview requests for a specific child, evaluating several critical factors in consultation with ACF and/or HHS before making a decision, ensuring programmed care remains central.
- Is the interview in the best interests of the child? (considering their placement, mental health, education, physical condition, culture, background, and family in the U.S.)
- Is the child represented by legal counsel? If so, does the attorney support the interview?
- Does the U.S. Department of Homeland Security (DHS) foresee potential adverse impacts on the child’s immigration case?
- Would the interview disrupt the facility or other children?
- Are special arrangements needed (e.g., interpreter, security)?
- How will the interview be conducted (e.g., video, phone)? What is the interview duration?
- Are there preferable alternatives to an interview?
Revised 08/01/2024
5.1.4 Requests to Visit a Facility
Media outlets may seek to tour a facility without interviewing children. To protect UC privacy, security, and well-being, media tours are generally not conducted when children are present. However, under specific circumstances, ORR will consider tour requests, evaluating the following factors in conjunction with ACF/HHS to ensure programmed care is not compromised:
- To what extent would the visit disrupt the facility or children?
- Are special arrangements required (e.g., security)?
- How will the tour be conducted (e.g., staff interviews, reporter numbers)? What is the tour duration?
- Are there preferable alternatives to a facility visit?
Revised 08/01/2024
5.1.5 Requests for General Information and Data
Media inquiries for general program data, such as UC numbers, nationalities, and backgrounds, are common. ORR publishes a wide range of data on the ACF website, including program size, origin country statistics, and county-level data for areas with significant UC releases. Grantees can always direct media to this resource: www.acf.hhs.gov/programs/orr/programs/ucs/about. ORR does not disclose UC names or private identifying information and generally prohibits photography or video that could reveal a child’s identity. ACF and/or HHS can provide approved facility images and, in some cases, videos for media use.
Revised 08/01/2024
5.2 ORR Policies on Requests to Tour ORR Care Provider Facilities
Parties interested in touring a care provider facility must submit a tour request through ORR. ORR evaluates these requests based on criteria outlined in Section 5.2.1 Evaluation Criteria, with the child’s best interests as the primary consideration in our programmed care model.
A tour involves a guided presentation of the physical ORR care provider facility by program staff. Tours do not include interactions with children unless explicitly pre-approved. Tour requests may come from advocacy groups, faith-based organizations, researchers, government officials, and other relevant stakeholders.
A visit refers to authorized meetings with specific children in ORR care, without a facility tour. Visit requests may be made by family members, potential sponsors, legal representatives, child advocates, or consulate officials.
- For family member and potential sponsor visit policies, see Section 3.3.10 Calls, Visitation, Mail, and Email.
- For consulate official visit policies, see Section 5.4.4 Visitation.
- Litigation-related visits must be arranged through ORR’s Division of Unaccompanied Children Policy.
Tours are generally not approved for attorneys, except for plaintiff’s counsel in existing settlements under settlement terms. Attorneys interested in providing legal services for UCs should contact UC Legal Services at [email protected].
For media requests, refer to Section 5.1 Responding to Inquiries from the Media.
Revised 9/18/2023
5.2.1 Evaluation Criteria
ORR uses the following criteria to assess tour requests, upholding the principles of programmed care:
- The requestor must have a legitimate mission or business purpose for the tour (e.g., state/local government matters, child welfare advocacy, legal issues).
- The tour must not adversely affect the privacy and well-being of children at the facility.
- Sufficient staffing and resources must be available to conduct the tour while protecting UC privacy and well-being. Visitor numbers are also considered.
- Adequate notice is required. Requests should be submitted two weeks prior to the tour. Requests with shorter notice may be considered under exigent circumstances.
Revised 9/18/2023
5.2.2 Special Arrangements
Certain tours may require special arrangements, such as enhanced security or accessibility provisions. These needs must be specified in the tour request and coordinated prior to approval. Requests for access to specific individuals, such as staff or children, will be coordinated with the ORR/Federal Field Specialist (FFS). ORR will only approve such requests if they align with the best interests of the child within our programmed care framework.
Revised 9/18/2023
5.2.3 Protocol for Tours of Care Provider Facilities
All parties seeking to tour an ORR care provider facility must submit the Unaccompanied Child (UC) Tour Request Form to [email protected]. Litigation-related tours must be arranged through ORR’s UC Policy Unit. Flores Council visits are coordinated via the U.S. Department of Justice and the ORR/Federal Field Specialist (FFS), following ORR procedures.
All tours must be conducted in a manner consistent with ORR’s legal and child welfare obligations, treating all children with dignity, respect, and sensitivity to their vulnerability as unaccompanied minors. This is a core tenet of our programmed care approach.
Approved participants may tour standard, secure, and emergency influx facilities. Tours must comply with ORR policies and procedures, as well as the internal policies of the specific care provider facility.
The maximum tour group size is six adults, including interpreters and support staff. Each participant must identify their professional connection to the UC Bureau’s mission and any affiliated organizations. Visitors not pre-identified may not be accommodated.
Tour Requirements:
- Tours must occur during normal business hours and last no longer than 1.5 hours.
- Tours must minimize disruption to the facility’s normal operations.
- Tours must not interrupt routine activities, such as mealtimes or scheduled programs.
Tour Participant Responsibilities:
- Be mindful of staff responsibilities.
- Remain with their ORR federal guide at all times.
- Refrain from interacting with staff or children unless specifically pre-approved.
- Exhibit appropriate adult role-modeling, showing respect and empathy toward staff and others, as children may be observing.
- Respect UC and staff privacy, including personal effects and documents.
- Do not search cabinets, drawers, personal belongings, or other unauthorized areas that may contain sensitive UC information.
- Do not share identifying information, such as facility addresses, with non-tour participants.
Recording devices, including phones and cameras, are prohibited inside care provider facilities during tours.
ORR reserves the right to terminate a tour if any participant violates tour protocols, ORR policies, or facility policies.
Additional protocols or exceptions may apply to:
- Legal representatives (Flores counsel, legal service providers);
- Child advocates, including Protection and Advocacy Systems (P&A) (see Section 5.2.5 Protection and Advocacy System Visits);
- Consulate Officials;
- Members of Congress (Section 5.2.4 Congressional Visits);
- Groups conducting oversight and investigations (e.g., HHS Office of Inspector General, law enforcement).
Revised 9/18/2023
5.2.4 Congressional Visits
U.S. Members of Congress may tour ORR care provider and influx care facilities for oversight purposes, provided:
- Visits are coordinated with ORR at least two business days in advance to minimize program disruption and ensure child welfare and safety operations are not compromised. 1
- Members of Congress must present official government-issued photo identification upon request (e.g., Congressional ID card).
- Staff accompanying elected officials must show current identification from their legislative body confirming their official government role.
Congressional staff, unless accompanying a Member of Congress, must adhere to general tour requirements in Section 5.2 ORR Policies on Requests to Tour ORR Care Provider Facilities, including the two-week advance request requirement.
Revised 9/18/2023
5.2.5 Protection and Advocacy System Tours and Visits
Protection and Advocacy Systems (P&As) exist in each U.S. state, D.C., five territories, and for Native Americans in the four corners region, to protect the rights of individuals with disabilities. These independent systems offer legal representation, advocacy, and assistance to state/territory residents with disabilities.
P&As may seek reasonable unaccompanied access to standard and temporary emergency facilities for:
- Providing information, training, and referrals regarding disability rights and needs programs.
- Monitoring compliance with disability rights and safety.
- Inspecting areas used by or accessible to children with disabilities.
- Investigating facilities based on complaints or probable cause of abuse or neglect.
Facility Access
Facility access for P&As must be reasonable and granted immediately upon request. Advance notice is reasonable for informational and advocacy purposes but is optional for monitoring, inspection, and investigation. For investigations due to complaints or probable cause of abuse/neglect, unaccompanied access may occur outside of business hours at the P&A’s discretion and without prior notice.
P&As have reasonable unaccompanied access to areas used by or accessible to individuals with disabilities within standard or temporary emergency facilities and may inspect, view, and photograph these areas.
Access to Children with Disabilities
Care providers must provide reasonable unaccompanied access to any individual with a disability in ORR facilities, as part of programmed care for vulnerable populations.
Unless responding to abuse/neglect complaints or probable cause, P&As should schedule child interviews in advance at reasonable times that do not disrupt daily routines. Children may refuse or end interviews at any time.
P&As may not photograph or video record residents without consent.
Response to Complaints with Probable Cause
P&As are not required to provide advance notice for visits related to abuse/neglect complaints or probable cause.
P&As may interview any UC, resident, employee, or other person reasonably believed to have knowledge of the incident under investigation. Children may refuse or terminate interviews at any time.
Access to Records
ORR will provide P&As access to UC records when authorized and appropriately requested under federal regulations governing disclosures to P&As. P&As must adhere to strict confidentiality requirements, and collected records must not be misused or inappropriately disseminated.
P&As must conduct activities to minimize facility program interference, respect UC privacy, and honor a child’s request to end an interview. P&As must follow Section 5.2.3 Protocol for Tours of Care Provider Facilities, except for explicit instances mentioned in this section (unaccompanied access, photography/video of facility areas used by children, and record access).
Posted 9/18/2023
5.3 Testimony by Employees and Production of Documents Where the United States is Not a Party
Information on requesting ORR employee testimony or document production in cases where the U.S. is not a party is available at 45 CFR Part 2 . This section ensures consistent legal procedures within the programmed care framework.
Posted 3/30/2015
5.3.1 Care Provider Testimony and Views
ORR care provider staff should follow their organization’s policy regarding testimony, which may include consulting with the care provider’s attorney. If staff members testify, they must clarify that they do not represent ORR and their testimony does not reflect ORR’s opinion or position.
Posted 3/30/2015
5.3.2 Confidentiality of Information
Care providers must maintain UC information confidentiality and protect it from unauthorized disclosure, a crucial aspect of programmed care. Generally, client information should not be revealed in affidavits or testimony unless legally required and with ORR approval. However, UCs aged 14 and older who wish staff to testify or provide a declaration may consent in writing, after which ORR could approve confidential information disclosure.
For children under 14 or lacking capacity to consent, care providers should seek written consent from the child’s parent or legal guardian to include confidential information in affidavits or testimony. If such consent is unavailable, ORR should be contacted.
Posted 3/30/2015
5.3.3 Prohibition on Release of Records Without Prior Approval
UC case file records are ORR property, regardless of possession location (ORR, care provider facility, or Post-Release Services (PRS) provider). Subject to whistleblower protections, care providers and PRS providers must not release these records or information without prior ORR approval, except for program administration purposes. This does not apply to Child Advocates, who have access to client case file information and can request copies directly from care providers without standard ORR request processes, as per Section 5.10.3 Information Sharing with LSPs, Attorneys of Record, and Child Advocates.
Revised 08/01/2024
5.4 ORR Policies on Communication and Interaction with Consulates
ORR and its care providers must adhere to consulate notification protocols under international and federal law. In most cases, ORR must notify a UC’s consulate of their custody and care provider facility location. UCs must have reasonable access to consulate officials and, in some instances, may be required to meet with them at the consulate’s request. ORR policies cover notification, access, visitation, and documentation of consulate interactions, ensuring programmed care includes international legal obligations.
Revised 9/18/2023
5.4.1 Notifications to Consulates
Q1: How does ORR notify consulates when their citizens are in ORR custody?
A1:
- Children from countries requiring mandatory notification[2](#foot2)
- For children from mandatory notification countries, care providers, with ORR/FFS collaboration, must notify the consulate as soon as practically possible, even against the child’s wishes. Notification is required even if the child claims credible fear or seeks asylum; however, credible fear or asylum claims must not be disclosed to the consulate under any circumstances.
- Children from countries NOT requiring mandatory notification
- For children from non-mandatory notification countries, consulate notification is not required. However, if a consulate or region formally requests standing notification for its citizens, ORR may instruct care providers to provide notice under mutually agreed terms. Agreements may specify notification frequency and information provided, balancing consulate information needs with ORR program effectiveness and UC privacy. Even with agreements, care providers and ORR/FFS must not share the name or any information about a child claiming credible fear or asylum from a non-mandatory notification country.
Posted 4/27/2015
5.4.2 Unaccompanied Alien Children’s Right to Contact and Visit with their Consulate
During admission orientation (within 48 hours of arrival), care providers must inform UCs of their right to contact their consulate and provide telephone access and consulate contact information. If a UC requests a consulate visit, the Case Manager will arrange a visit at the care provider facility with the consulate. This is a standard part of programmed care orientation.
Revised 9/18/2023
5.4.3 Consulate Officials: Access to Their Citizens and ORR Care Provider Facilities
Consulate officials seeking to meet with a UC must request access through the child’s case manager. Access depends on whether the child is from a mandatory or non-mandatory notification country. This protocol is designed to ensure respectful and programmed care interactions.
- Children from countries requiring mandatory notification:
- For children from mandatory notification countries, care providers must arrange visits as soon as reasonably possible, regardless of the child’s wishes to meet or not. This applies even if the child claims credible fear or seeks asylum.
- Children from countries NOT requiring mandatory notification:
- For children from non-mandatory notification countries, care providers must attempt to contact the child’s parent or legal guardian to seek permission for a consulate visit.3 If the parent/legal guardian is unavailable or unresponsive within 72 hours, the visit may be presumed authorized, unless the child objects or claims credible fear/asylum, in which case, access must be denied.
Facility Tours for Consulate Officials: Consulates seeking to tour ORR care provider facilities or meet program staff must submit a UC Tour Request Form to [email protected]. Refer to Section 5.2 ORR Policies on Requests to Tour ORR Care Provider Facilities for more information on tour requests.
Consulate Officials Bringing Additional Adults: If consulate officials wish to bring non-consulate officials (e.g., foreign dignitaries, third parties) on tours, they must include all tour participants in the tour request, adhering to ORR facility tour policies in Section 5.2 ORR Policies on Requests to Tour ORR Care Provider Facilities, including the six-adult limit per tour request. ORR will evaluate the request based on policy criteria.
Revised 9/18/2023
5.4.4 Visitation
Case Managers will arrange consular visits, providing private meeting spaces for consulate officials and UCs. Visits will follow care provider time, place, and manner restrictions to minimize facility operation disruptions, maintaining consistent programmed care routines.
Posted 4/27/2015
5.4.5 Information Requests
If consulate officials request information on UCs in ORR care beyond placement confirmation, they must submit a request to ORR. ORR may approve or deny requests at its discretion, considering information availability and UC privacy concerns. Generally, ORR does not release private information, such as medical and mental health records, without the child’s consent.
Posted 4/27/2015
5.4.6 Documentation
Care providers must maintain documentation in individual UC case files regarding access requests and meetings between UCs and their consulates. Case Managers must document this information in Case Manager notes. Care providers must also maintain records of general consulate visits or requests not specific to individual children, ensuring comprehensive record-keeping within programmed care.
Posted 4/27/2015
5.4.7 ORR and Consulate Joint Activities
ORR partners with foreign consulates in several areas, enhancing programmed care through international cooperation:
- Foreign document authentication: Consulates assist in authenticating foreign documents like birth certificates, aiding age determinations and establishing familial relationships for potential sponsors.
- Family tracing: Consulates help Case Managers facilitate communication between UCs and their families in their home countries, especially when families are in remote areas or are unknown, or when children are too young to communicate effectively.
- Information provision related to crimes: Consulates may assist ORR in locating information about crimes where a UC may be a perpetrator, witness, or victim in their home country. This information informs ORR placement, service, and release decisions.
Posted 4/27/2015
5.5 ORR Monitoring and Compliance
This section covers ORR’s monitoring activities, staff roles, foster care monitoring, and care provider internal monitoring. ORR conducts at least monthly monitoring visits to ensure care providers meet minimum standards for UC care and timely release, adhering to all federal/state laws, licensing/accreditation standards, ORR policies, and child welfare standards. Monitoring frequency increases if warranted by facility issues. Non-compliance findings result in corrective action requirements and deadlines. ORR also provides technical assistance to address deficiencies, maintaining the integrity of programmed care.
Corrective action is central to ORR’s monitoring policy and can be issued anytime through various monitoring activities. The ORR team’s expertise allows field staff to report on-site findings (licensing, specific UC cases) and Grants Management staff to evaluate budget, program management, and risk assessment issues.
ORR’s primary goal is UC care and safety. Therefore, ORR may discontinue funding, halt placements, remove children, and/or close programs failing to address corrective actions effectively and promptly. Notification procedures and monitoring activities ensure immediate responses to safety and security issues.
Revised 08/01/2024
5.5.1 ORR Monitoring Activities
ORR monitoring is an ongoing, multi-layered process providing consistent oversight across all program components: program design, management, services, safety, security, child protection, case management, personnel, stakeholder relations, and fiscal management, ensuring consistent programmed care quality. Monitoring policies in this section establish formal accountability standards and checkpoints at regular intervals.
ORR monitoring activities include:
- Desk Monitoring: Ongoing oversight using the HHS grants management model, including monthly check-ins with the care provider’s ORR/Project Officer (PO), regular record/report reviews, financial/budget analysis, and communications review.
- Routine Site Visit Monitoring: Monthly or bi-monthly day-long facility visits (announced and unannounced) to review policies, procedures, practices, and guideline compliance, typically focusing on case management services.
- Site Visits in Response to PO or Other Requests: Targeted visits for specific purposes or investigations, such as corrective action plan follow-up.
- Monitoring Visits: Comprehensive week-long site reviews conducted at least every two years.
Desk Monitoring: ORR Division of Grants Management staff conducts ongoing desk monitoring, including regular reviews of records and reports (annual goals/objectives, quarterly program reports, Significant Incident Reports (SIRs), ORR case management database usage reports, and financial reports). Regular calls with care provider Program Directors and others provide insight into program infrastructure and management systems and review data from required documents and reports. ORR staff also request and spot-check facility case files for policy/procedure compliance and SIR follow-up.
Routine Site Visits: ORR staff conducts routine day-long site visits at least monthly at each facility to observe service delivery and review records/procedures. During visits, ORR representatives attend “case staffings” (meetings discussing individual UC cases with care provider staff, Case Coordinators, etc.) to observe team collaboration and case management system effectiveness. Monthly facility reports and quarterly reports identifying strengths, weaknesses, concerns, and training needs are generated based on site visit findings.
Safety or security concerns or issues requiring escalation from desk monitoring or site visits are immediately reported to ORR supervisors.
Monitoring Visits: Monitoring visits, conducted at least every two years, involve comprehensive inspections based on pre-visit information, on-site reviews, and interviews with staff, UCs, and stakeholders. Formal monitoring visits use templates, checklists, and other tools completed at each site. A monitoring report with corrective actions is submitted to the provider within 30 days of the visit. Corrective actions address non-compliance with explicit ORR policies/procedures. Providers must submit a corrective action plan response within 30 days, detailing corrective measures and timelines. ORR may require more immediate action when necessary.
Before monitoring visits, care providers must provide written responses to standardized questions about operations (Site Visit Guide), including internal quality assurance, child protection, case management, health, education, services, administration, and financial management practices. Providers also submit documents to ORR before and during visits.
Relevant documents, reports, and files reviewed include:
- Grant application/cooperative agreements
- Completed Site Visit Guide responses
- Recent facility staff organizational chart
- Educational curriculum and weekly class schedule
- Food services/menus and employee food safety certifications
- Facility lease
- State and local licenses, licensing requirements (or links), and recent state licensing inspection reports
- Recent Audit Report and Financial Status Report
- Recent vehicle inspection
- Safety and sanitation certificates—Fire inspection report
- Quality assurance procedures and internal monitoring resources
- Most recent Quarterly Report
- Current approved Fiscal year budget
- Recent SIRs
- Previous monitoring visit reports (including corrective action plans) and site visit reports
- UC case files
- Care provider staff personnel files
- Care provider’s internal policies and procedures
- Care provider’s grievance policy and UC grievances
- Materials/reports on timely and accurate ORR case management database use
Week-long monitoring visits include standardized interviews with lead teams for each program component (e.g., Lead Teacher, Lead Clinician), Program Director, stakeholders (Legal Service Provider, Case Coordinator, Medical Provider, non-HHS Federal agency partners, etc.), and UCs. Thorough physical facility inspections are also conducted. Care providers must comply with ORR requests for facility access, program information, and case files during any monitoring activity, supporting programmed care oversight.
Each site visit generally involves reviewing 3-15 randomly selected case files and related documentation, personnel files, related documents from the list above, and submitted SIRs and internal incident reports.
In secure care facilities, Monitoring POs review Further Assessment Swift Track (FAST) Assessment information in case files to ensure children in secure care are assessed every 30 days for potential transfer to less restrictive settings, ensuring appropriate programmed care levels.
Monitoring POs consult with assigned Project Officers, Federal Field Specialists, Case Coordinators, CFS, and DHUC Quality Assurance Specialists and meet with POs and FFS to discuss findings and trends.
ORR monitoring and compliance responsibilities are divided among teams in the table below, working collaboratively and independently for enhanced scrutiny and focused attention.
Roles and Responsibilities in ORR Monitoring and Compliance Model
| Team | Responsibilities | Time Frame |
|---|---|---|
| ORR Monitoring Team: Project Officers dedicated to monitoring and compliance, overseeing program management, services, safety, security, child protection, case management, personnel management, and fiscal management. | Reviews policies, procedures, reports, and case files; conducts 5-day facility visit and inspection to review additional reports/case files/documents, interviews staff, children, and stakeholders. Issues monitoring report (30 days post-visit) documenting corrective actions. Care providers must respond with a corrective action plan within 30 days. | Every two (2) years |
| Contractor Field Specialist (CFS) Team: Conducts independent site visits to all care provider facilities to provide technical assistance and identify deviations from ORR policies and procedures. | Routine site visits to every care provider (each CFS assigned to specific providers) for firsthand facility observation. Visits may be announced or unannounced. CFS provides ORR monthly reports on findings and quarterly reports summarizing facility strengths, weaknesses, concerns, and training needs, with emphasis on case management services. CFS immediately reports issues requiring escalation to regional FFS supervisor and assigned PO. | Monthly or twice a month to every care provider |
| ORR Project Officer (PO) Team: Project Officers oversee specific care provider facilities, escalating issues arising from day-to-day oversight. | Conducts ongoing desk monitoring by reviewing all required documents and reports. POs are responsible for overseeing care provider implementation of corrective action plans. | Ongoing; Monthly conference calls with assigned care providers. |
| ORR Federal Field Specialist (FFS) Team | As local ORR liaisons with care providers and stakeholders, FFS are ORR’s “eyes and ears” on the ground in specified regions, serving as regional approval authority for transfer and release decisions. FFS may issue corrective actions (along with Program POs and Monitoring POs). | Ongoing |
Posted 08/01/2024
5.5.2 Follow Up and Corrective Actions
Non-compliance findings from ORR monitoring activities result in written communication to the Program Director or appropriate personnel via a monitoring or site visit report, including corrective actions and child welfare best practice recommendations. Corrective actions are required when care providers are non-compliant with explicit ORR policies and procedures, ensuring consistent programmed care standards.
The following table outlines corrective action team responsibilities, ensuring comprehensive review across all areas for each care provider.
| Individual Issuing Corrective Action | Areas Covered |
|---|---|
| ORR Project Officer | – Program Design – Personnel – Compliance with ORR Policy and Procedures – Budgetary impact items – Staffing Ratios Compliance with grants terms and conditions – Licensing Standards Compliance – Unaccompanied Child Safety/Risk Issues |
| ORR FFS | – Compliance with ORR Policy and Procedures – Unaccompanied Child Safety/Risk Issues – Licensing Standards Compliance – Child Specific Issues |
Following corrective action issuance, the ORR/Project Officer (ORR/PO) or ORR/Federal Field Specialist (ORR/FFS) requests a corrective action response from the Program Director, determining resolution timeframes and disciplinary consequences for non-response within required timeframes.
Care provider corrective action plans must include:
- Cause of non-compliance (essential for effective corrective action).
- Clear and concise corrective action statements (including responsible parties and timelines).
- Thorough corrective action descriptions referencing specific documents, procedures, etc.
- Corrective action completion date.
- Evidence supporting full and effective corrective action implementation, performed as described.
For information on grant termination and enforcement, see 45 CFR Part 74 .
Posted 6/15/2015
5.5.3 Foster Care Monitoring
Care providers offering UC care through foster care sub-contracts or sub-grants are responsible for annual sub-recipient monitoring or site visits and weekly desk monitoring. This includes evaluating sub-recipient compliance with applicable federal, state, and local laws, upholding programmed care standards across all settings. Care providers must provide review findings to the designated ORR/Project Officer (ORR/PO) upon request.
ORR assesses care providers with foster home arrangements via on-site and desk monitoring and may also conduct foster home monitoring as needed.
Care providers with foster home arrangements are subject to the same monitoring schedule as other care provider facilities, but activities are tailored to foster care arrangements. ORR Monitors may schedule visits with grantee staff and foster homes during on-site monitoring visits for firsthand home environment and care provider oversight assessments.
Posted 6/15/2015
5.5.4 Abuse Review Team
In addition to routine monitoring, ORR’s Abuse Review Team (ART) rapidly reviews serious or egregious abuse allegations. The team comprises ORR staff with relevant expertise, including Monitoring Team members, the Division of Health for Unaccompanied Children, and ORR’s Prevention of Sexual Abuse Coordinator, ensuring specialized programmed care oversight.
The ART evaluates and desk-monitors all allegations in the categories below. ORR leadership may also request ART review of other abuse allegations of particular concern.
- Sexual abuse of a UC by staff or other adult (45 CFR 411.6 definition).
- Sexual abuse of a UC by another UC (45 CFR 411.6 definition), excluding intentional touching allegations.
- Physical injury of a UC by staff or another UC, including lacerations, fractures, burns, internal injuries, severe bruising, or serious bodily harm.
- Negligent UC treatment, including failure to provide adequate food, clothing, or shelter, seriously endangering physical health.
- Inappropriate discipline use, including corporal punishment, resulting in humiliation, mental abuse, or punitive interference with daily functions (eating, sleeping).4
- Negligent UC treatment, including failure to provide routine/urgent medical, mental, or dental care and necessary medications, seriously endangering physical or mental health.
- Inappropriate health intervention use, including quarantine, isolation, physical/chemical restraints, or delayed discharge.
In addition to desk monitoring, the ART may identify necessary measures to ensure UC safety at the care provider facility where the allegation occurred. These measures may include:
- On-site monitoring by ART members.
- Corporate office monitoring to review internal policies, reporting structures, and supervisory responses.
- Limiting new UC placements at the facility.
- Stopping placements at the facility.
- Removing all UCs from the facility and placing them in other local facilities.
- Issuing corrective actions.
- Closing the care provider facility.
Revised 08/02/2023
5.5.5 Care Provider Internal Program Monitoring, Evaluation, and Quality Assurance
Care provider facilities must have internal monitoring processes, set by their organization and professional accreditation/licensing agencies, ensuring continuous programmed care improvement.
Care providers are expected to conduct internal monitoring, evaluation, and continuous quality assurance assessments quarterly to identify areas needing improvement or modification. The plan must evaluate how the facility:
- Complies with federal/state laws, ORR policies/procedures, and state/local licensing requirements, including programs ineligible for state/local licensing.
- Fulfills program cooperative agreement/contract and ORR Statement of Work terms.
- Identifies corrective action plan issues.
- Meets affiliate accreditation agency requirements, if applicable.
- Provides for timely UC processing and release.
Care providers must evaluate program strengths and weaknesses based on performance indicators:
- Number/type of UC and staff grievances.
- Adverse state/local licensing citations.
- Staff misconduct allegations and findings.
- On-site accidents.
- Restraint use.
- Timeliness of service delivery and UC discharges.
- Corrective action plan activities, if applicable.
Revised 08/01/2024
5.6 Reporting and Record Keeping
ORR-funded care providers submit quarterly and annual performance and financial status reports and comply with other program integrity and accountability measures, ensuring transparent programmed care operations.
Revised reports must be submitted by the indicated due date. Failure may result in immediate corrective action or other enforcement measures.
Posted 7/27/2015
5.6.1 Program Reporting Requirements5
| Type of Report | Reporting Requirements | Time Frame |
|---|---|---|
| Performance Progress Reporting | In accordance with grant or contract terms. SS-PPR ACF Performance Progress Report (PPR) | Quarterly basis, starting October 1, to ACF Office of Grants Management and ORR PO |
| Financial Reporting | SF-425 Federal Financial Report (FFR), reflecting cumulative actual Federal funds, unliquidated obligations, and unobligated balances. (Note: FFRs are federal government claims; false claims may result in civil/criminal penalties.) Supporting SF-425 documentation may be requested. | Within 30 days after each quarter’s end to ACF Office of Grants Management and ORR PO. Revisions required for SF-425 discrepancies. |
| Program Reports | Additional programmatic or statistical information upon ORR request (one-time or ongoing). | As specified by ORR. Care providers must seek timely clarification if needed. |
Posted 7/27/2015
5.6.2 Maintaining Case Files
Care provider facilities and post-release services (PRS) providers must maintain comprehensive, accurate, and up-to-date case files and electronic records on children, kept confidential and secure at all times and accessible to ORR upon request. (Case file records may be hard copy and/or electronic on provider networks and ORR case management system.) Care providers must have written policies/procedures for organizing and maintaining active/closed case file content, incorporating state licensing/accrediting agency requirements and ORR policies/procedures, ensuring meticulous programmed care documentation.
To ensure accurate recordkeeping and quality UC care, care providers must create individual case files for each child, including name, A number, service dates, and federal fiscal year. Files document all services, UC progress, barriers, and case outcomes.
Each UC case file must minimally include:
Unaccompanied Child Information
- Name and A Number
- Birth certificate
- Photograph
Placement Documents
- Placement Authorization
- Intakes Placement Checklist
- Property and cash inventory (child-signed)
- Clothing and supplies list
- Placement in Restrictive Setting Notice (if applicable)
- Child acknowledgment of orientation (program rules/policies, self-disclosure notifications, grievance procedures, boundaries, abuse/neglect, emergency/evacuation procedures) in their language
- Child acknowledgment of local/national service provider and organization information (local child advocacy centers, rape crisis centers, immigrant victim service providers, community service providers for sexual abuse/harassment victims at the facility)
Legal Information
- Acknowledgment of Legal Resource Guide receipt at admission and discharge
- Executive Office of Immigration Review (immigration court) documents, including risk determination hearing documents
- Notice to Appear (U.S. Customs and Border Protection issued, if applicable)
- Court documents/criminal history records (if applicable)
- Authorization for Release of Records (if applicable)
Medical Records
- Authorization for Medical, Dental, and Mental Health Care
- Initial Medical Exam documentation
- Medical service referral copies
- Medical and mental health records (including over-the-counter medications), diagnoses, and communicable disease documentation
- Lab results and imaging studies (CT scans, X-rays, MRIs)
- Immunization Records
- Prescriptions (including logs)
- Dental exam records
- TB Screening results
- Office visit/ER visit/hospital/surgery records
- Progress notes related to medical or mental health services (if applicable)
- Diagnosis list
Educational Services
- Educational assessment summary
- Individualized Education Program (IEP), if applicable
- Education plan (class placement, curriculum/course descriptions, academic reports, progress notes)
Case Management Records
- Case manager progress notes
- Recreation/activity log
- Telephone log
- Religious services log
- Stipend log (if state licensing mandated)
- Individual Service Plan (ISP) and updates
- Sponsor Assessment
- Family Reunification Packet
- Home Study Report
Clinical/Mental Health Records
- Individual counseling session progress notes
- Group counseling notes/records
- Mental health services progress notes (if applicable)
- Mental health assessments (if applicable)
- Mental health office visit, telepsychology/psychiatry/psychotherapy session, or hospitalization records (if applicable)
- Psychotropic prescriptions, including logs (if applicable)
- Initial Intakes Assessment
- Assessment for Risk
- UC Assessment
- UC Case Review and updates
- Disclosure Notice for counseling services
- Behavioral Notes (if applicable)
- Historical Disclosures (if applicable)
Incident Reports
- Significant Incident Reports (if applicable)
- Facility Internal Incident documentation/reports
- Grievances/Grievance Reports
Discharge/Exit Information
- Verification of Release form
- Transfer Request and Tracking form
- Notice of Transfer to ICE Chief Counsel (Change of Address/Change of Venue) (transfers only)
- Discharge document/checklist log
- Property return/disbursement log
- Medical record discharge checklist
- Copy of Removal Order (if applicable) (see Legal Information)
- Copy of Trafficking Eligibility Letter (if applicable)
Care providers must ensure compliance with federal statutes concerning personal identifying information collection and maintenance in case file preparation and management.
Revised 08/01/2024
5.6.3 Record Management, Retention and Safekeeping
Care providers must ensure all records are maintained and protected for confidentiality and data security, preventing unauthorized access, use, disclosure, or improper alteration. Administrative and physical controls must prevent unauthorized access to electronic and paper records, a critical aspect of programmed care data management. Electronic records (including ORR case management database records) cannot be accessed outside the U.S. Care providers’ internal policies must align with ORR’s policy prohibiting ORR case management database use outside the U.S. Policies and procedures must also address preventing physical record damage or destruction. Sensitive UC information (sexual abuse, clinical records) requires appropriate dissemination controls to prevent misuse by staff or other children.
Care providers are also responsible for timely entry of all required information into the ORR case management database. For specific timeframes related to UC and sponsor assessments, reporting, and release, see:
Section 2.2.3 The Family Reunification Application Section 3.3.1 UC Assessment and Case Review Section 3.4.2 Initial Medical and Dental Examinations and Follow-up Care Section 3.4.5 Responding to Medical Emergencies Section 4.8.1 Assessment for Risk Section 2.8.2 Transfer of Physical Custody Section 2.8.3 Closing the Case File
Care providers must provide timely and unrestricted file access to ORR or ORR-designated entities.
Care providers must establish internal file review systems for periodic (minimum quarterly) individual case file completeness and accuracy reviews.
ORR will determine case file and program information retention/disposition procedures before grant/contract end. Case files must be stored for the longer of state licensing/accrediting agency standards or three years (five years for ORR case management database records) from UC release date. (Litigation cases must be maintained until case resolution.)
Complete closed case files may be scanned and saved electronically if state licensing regulations permit. Care providers must state record retention timeframes in internal policies/procedures, complying with ORR requirements, state licensing regulations, and/or accrediting agency requirements.
Once record retention terms mature, care providers must inform ORR and seek disposal/transfer guidance. Care providers must never destroy, keep, or transfer records without prior ORR authorization.
Active and closed case files must be kept in locked cabinets when not in use. At a minimum, care providers must ensure:
- Records (paper and electronic) are protected from public access.
- Paper record/electronic storage areas are supervised and/or securely locked during business hours to prevent unauthorized access.
- Records are inaccessible to unauthorized persons.
- Records are not shared with unauthorized persons or under unauthorized circumstances (oral or written).
- Safeguards are in place to prevent document misuse.
- All care provider sub-contractors, consultants, and outside parties are prohibited from using or disclosing program information for purposes outside governing contracts/agreements.
- Sub-contractors/consultants return all ORR documents or destroy non-ORR documents upon contract completion.
- ORR consent is obtained prior to destroying any documentation (disposable documents must be shredded or properly disposed of by reputable companies).
Posted 08/01/2024
5.7 ORR Policies to Protect Sponsors from Fraud
ORR does not charge fees to prospective or approved sponsors as a UC release condition. Payment demands are unauthorized and should be disregarded. This policy protects the integrity of programmed care and family reunification.
Prospective sponsors should immediately report suspicious calls or payment requests to the care provider facility, ORR directly, or the ORR National Call Center Help Line at 1 (800) 203-7001.
Posted 7/27/2015
5.7.1 ORR Efforts to Help Prevent Fraud
Care providers inform all potential sponsors that ORR, its care providers, volunteer agencies, and grantees/contractors do not collect fees for UC release services from HHS custody.7
To detect potential fraud schemes, ORR also asks all approved sponsors at UC release if anyone has requested money during the release process.
The FBI recommends public caution and adherence to these guidelines before payment/donation:
- Be skeptical of individuals claiming to be officials and requesting payments/donations door-to-door, via phone, mail, email, or social media.
- Be skeptical of payment/contribution requests via courier or wire, or requests for bank account or credit card numbers.
- Verify government agency/non-profit legitimacy using internet resources to confirm phone numbers, emails, group existence, and non-profit status, rather than following email links.
- Call official government agency phone numbers to verify payment request legitimacy.
- Do not respond to unsolicited (spam) emails or click links within them.
- Be cautious of emails with picture attachments of intended recipients, which may contain viruses. Only open attachments from known senders.
- Make contributions directly to known organizations, ensuring intended use.
- Do not provide personal or financial information to payment/contribution solicitors, which may compromise identity and lead to theft.
See New Fraud Schemes Targeting Families of Unaccompanied Children for Spanish translation.
ORR also requests sponsors to:
- Report suspicious calls/contacts to care provider facilities and ORR directly.
- Call the ORR National Call Center Help Line at 1 (800) 203-7001 to report fraud or attempted fraud.
Posted 7/27/2015
5.7.2 Responding to Fraud Attempts
If a care provider determines a sponsor or prospective sponsor is a fraud target, they must report the incident to ORR via a Significant Incident Report (SIR) and to local law enforcement, maintaining vigilant programmed care and safety protocols.
ORR reviews SIR information and reports all fraud schemes (attempted or successful) to HHS/Office of the Inspector General (OIG). ORR and care providers may consult with HHS/OIG on investigations, providing circumstantial information and clarifications after SIR submission. HHS/OIG case file record requests require an Authorization for Release of Records form, following the process in Section 5.10.1 UC Case File Request Process. Requests may be expedited at ORR discretion under Section 5.10.1 criteria.
If fraud schemes involve care provider staff, ORR instructs care providers to contact local law enforcement and follow local licensing guidelines for inappropriate employee behavior reports, informing licensing agencies of HHS/OIG and law enforcement referrals. Care provider facilities must take disciplinary action, including staff termination for criminal behavior, including fraud. ORR issues corrective action findings and requires appropriate care provider action (see Section 5.5.2 Follow Up and Corrective Actions).
Revised 08/07/2023
5.8 Reporting Child-Level and Program-Level Events
ORR requires care providers and staff to report incidents affecting UC safety/well-being and record observations to inform best needs management, ensuring responsive programmed care. Care providers must report a wide range of incidents/observations, including staff abuse/neglect, UC property destruction, mental health concerns, and program-affecting natural disasters.
 flowchart
flowchart
Reporting these events to ORR ensures documentation and appropriate responses to significant UC incidents, protecting their best interests, safety, and well-being. Incident reports are primarily internal records for immediate ORR awareness, not comprehensive UC care records or legal/medical/clinical/decision documents. Information may be unverified, and incident responses may be ongoing. Incident reports are not intended to provide complete context (trauma, other incidents, UC history).
Care providers must never threaten UCs with incident/event reporting for behavior control or any other reason. Significant Incident Reports (SIRs) cannot be the sole basis for UC step-up to restrictive placements, step-down refusal, or facility placement refusal.
This section details each event category, reporting requirements, reference charts, and instructions for notifying non-governmental stakeholders (attorneys, potential sponsors, etc.).
Some events constitute emergencies, requiring prompt ORR notification and Emergency SIR form completion (see Section 5.8.1 Emergency Incidents).
Non-emergency significant incidents require SIR form reporting via the ORR case management database (see Section 5.8.2 Significant Incidents).
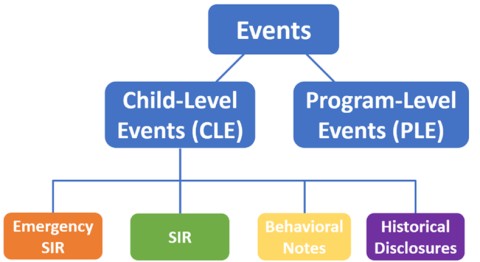
Child-level events (CLE) affect individual children (emergency incidents, significant incidents, behavioral notes, historical disclosures), with reporting requirements in Section 5.8.1, Section 5.8.2, and Section 5.8.12 Behavioral Notes and Historical Disclosures. Program-level events (PLEs) affect entire facilities and/or children/staff (active shooters, natural disasters), requiring PLE Report form submission via the ORR case management database (see Section 5.8.3 Program-Level Events).
Reports must include sufficient detail, sequential incident description, involved individuals, non-judgmental language, and follow-up actions. Proper incident documentation aids danger identification and prevention. In emergencies, significant incidents, or PLEs, UC and staff safety is prioritized over reporting requirements. See Section 5.5 ORR Monitoring and Compliance and Section 4.6 Coordinated Response for monitoring/compliance standards and ORR safety/well-being actions.
Reports cannot be provided to outside entities/individuals without prior ORR permission unless stated otherwise in policies/procedures. Notification emails to external entities about relevant incidents (mandatory reporting under law or ORR policy) must include the Significant Incident Report (SIR) Triage Team at [email protected].
Revised 08/01/2024
5.8.1 Emergency Incidents
Emergency incidents include (1) urgent situations with immediate and severe UC safety/well-being threats requiring immediate action, or (2) unauthorized absences, requiring immediate programmed care responses.
Emergency incidents include, but are not limited to:
- Abuse or neglect in ORR care with immediate and severe UC safety/well-being threat (physical assault with serious injury, sexual abuse, suicide attempt).
- UC death in ORR custody, including out-of-network facilities (see Section 3.3.16 Notification and Reporting of the Death of an Unaccompanied Child).
- Medical emergencies (see Section 3.4.5 Responding to Medical Emergencies).
- Mental health emergencies requiring hospitalization.
- Unauthorized UC absences (see Section 5.8.8 Reporting SIRs and Historical Disclosures to DHS for additional reporting).
Reporting:
Care providers must immediately report emergencies to 9-1-1, local law enforcement, Child Protective Services (CPS), HHS Office of the Inspector General, and state licensing agencies, as appropriate, under mandatory reporting laws, state licensing requirements, federal laws/regulations, and ORR policies/procedures. Facilities must also immediately report emergencies to the ORR/Federal Field Specialist (FFS) Supervisor. For unauthorized absences, care providers must automatically notify the legal service provider (LSP) or attorney of record (if applicable), and appointed Child Advocate (if any) within 48 hours.
Care providers must submit an Emergency Significant Incident Report (SIR) in ORR’s case management system within four (4) hours of an emergency incident (or awareness). Emergency SIRs must be filed for each UC involved, and multiple Emergency SIR Addendums may be needed for updated information after initial submission (see Section 5.8.4 Report Addendums).
Notification emails to external entities must include the SIR Triage Team at [email protected].
Revised 08/01/2024
5.8.2 Significant Incidents
Significant incidents are (1) situations that may immediately affect UC safety/well-being or (2) observations that may inform best UC care approaches, requiring diligent programmed care management.
Significant incidents include, but are not limited to:
- Abuse or neglect of a UC by an adult in ORR care.
- Sexual harassment or inappropriate sexual behavior.
- Staff code of conduct and boundary violations.
- External threats to children:
- Outside actors perpetrating actual/potential fraud schemes on UCs/sponsors.
- Human trafficking concerns/risks.
- Threats to UCs in ORR care related to crime/organized crime.
- Law enforcement incidents on-site at care providers.
- Outside actors perpetrating potential fraud schemes on UCs/sponsors.
- Intentional document/information fraud:
- UC or adult misrepresenting identity/age.
- Adult misrepresenting biological/familial relationship.
- Sponsor/potential sponsor misrepresenting identity/documentation.
- Sponsor/potential sponsor misrepresenting other children’s whereabouts/welfare (including former UCs in household).
- Sponsor/potential sponsor misrepresenting sponsor application information/supporting documentation.
- Sponsor/potential sponsor incorrectly reporting address, work status, or intended care plans.
- Healthcare errors.
- Pregnancy termination requests.
- Runaway attempts.
- Mental health concerns.
- Use of behavioral safety measures (restraints).
Reporting: Care providers must submit a completed SIR in ORR’s case management system within 24 hours of a significant incident (or awareness).
Care providers must also report significant incidents to CPS, state licensing, and/or local law enforcement, as appropriate, under mandatory reporting laws, state licensing requirements, federal laws/regulations, and ORR policies/procedures.
Note: ORR’s Integrity and Accountability Team (I&A) reports all fraud-related incidents to the HHS Office of Inspector General (HHS OIG). Care providers and field staff should not report fraud incidents to HHS OIG but must respond if HHS OIG requests circumstantial information/clarifications (see Section 5.7.2 Responding to Fraud Attempts) or use the case file request process for investigation records (see Section 5.10.7 Information Sharing with Investigative Agencies).
Some SIRs also require DHS notification (see Section 5.8.8 Reporting SIRs and Historical Disclosures to DHS).
An SIR must be filed for each UC involved in a significant incident, with SIR Addendums for updated information (see Section 5.8.4 Report Addendums). SIRs and addendums must be kept in UC case files.
Notification emails to external entities must include the SIR Triage Team at [email protected].
Revised 02/09/2024
5.8.3 Program-Level Events
Program-level events (PLEs) are situations affecting entire care provider facilities and/or children/staff, requiring immediate action and robust programmed care responses.
PLEs include, but are not limited to:
- Death of staff, other adults, or non-UCs at a care provider facility or foster home.
- Major disturbances (shooting/terrorist attack, riot, protest).
- Natural disasters (earthquake, flood, tornado, wildfire, hurricane).
- Any event affecting normal facility operations (long-term power outage, gas leaks, inoperable fire alarms, infectious disease outbreak8, intake/discharge stoppages, safety/abuse/neglect concerns where the child isn’t identified).
Reporting: Care providers must immediately report PLEs to 9-1-1, local law enforcement, CPS, and/or state licensing, as appropriate, under mandatory reporting laws, state licensing requirements, federal laws/regulations, and ORR policies/procedures. Facilities must also immediately report PLEs to the ORR/Federal Field Specialist (FFS) Supervisor.
Care providers must submit a PLE Report in the ORR case management database within four (4) hours of the event (or awareness)—or as soon as practicable. Follow-up reporting may be needed for multi-day or changing PLEs. Final PLE Reports are required after incident resolution.
If children are injured or become ill due to PLEs, and it rises to medical emergency levels (see Section 3.4.5 Responding to Medical Emergencies), SIRs must be filed for each child as outlined in Section 5.8.1 Emergency Incidents.
Notification emails to external entities must include the SIR Triage Team at [email protected].
Revised 08/02/2023
5.8.4 Report Addendums
Care providers must create addendums to Emergency Significant Incident Reports (SIRs) and SIRs when original document information is incorrect, incomplete, or new information emerges. Program-Level Event (PLE) reports should also be updated for incorrect, incomplete, or new information. Examples include sponsor discussions about incidents, media inquiries, and receipt of official reports from government agencies. This ensures accurate and evolving programmed care documentation.
Addendums to SIRs or PLE updates must be submitted to ORR within 24 hours of learning incorrect, incomplete, or new information.
Revised 6/7/2021
5.8.5 Elevation of Emergencies, Significant Incidents, and Program-Level Events
ORR elevates certain emergencies and significant incidents within its leadership structure as an additional protection measure, ensuring UC safety and appropriate care, and providing support to care providers and ORR field staff in complex situations, reinforcing robust programmed care oversight.
In the following cases, the ORR/Federal Field Specialist (ORR/FFS) must immediately elevate the case to their FFS Supervisor and the Significant Incident Report (SIR) Triage Team ([email protected]) simultaneously. The SIR Triage Team then elevates the case (keeping FFS and FFS Supervisor in the email) to the Field Manager, Director of the Division of Unaccompanied Children Policy, Associate UC Bureau Director, Manager of Project Officers and Grants Management, ORR Chief of Staff, Director of the Division of Planning and Logistics (DPL) (as applicable), Division of Health for Unaccompanied Children (DHUC) (as applicable), and the ORR Director.
- UC, staff, or other person death in a care provider facility or foster home.
- Situations with immediate danger to UC or staff lives (shooting/terrorist attack, natural disaster, medical emergency Section 3.4.5 Responding to Medical Emergencies, mental health emergency requiring hospitalization, potential infectious disease outbreak).
- Unauthorized UC absences.
- Any situation likely to require ORR leadership oversight or escalation to ACF/HHS leadership.
For facility-wide events (shooting/terrorist attack, natural disaster), the SIR Triage Team elevates the case to the DPL Director.
For UC deaths, medical emergencies, or mental health hospitalizations, the SIR Triage Team elevates the case to the DHUC Director.
In potential infectious disease outbreaks, ORR staff reports immediately to their supervisor, who elevates to DHUC. DHUC reviews and elevates confirmed outbreaks to the Field Manager, Division of Grants Management Manager, DPL Director, Director of the Division of Unaccompanied Children Policy, Director of the Division of Unaccompanied Children Placements, Director of the Division of Unaccompanied Children Field Operations, ORR Unaccompanied Children Bureau Deputy Director(s), ORR UC Bureau Chief, Deputy Assistant Secretary for Humanitarian Services, and ORR Director.
Quick Reference Chart: ORR Supervisor Requirements for Elevation of Emergencies, Significant Incidents, and Program-Level Events
Note: This chart is a quick reference and not exhaustive.
| TYPE OF INCIDENT | CARE PROVIDER REPORTING REQUIREMENTS |
|---|---|
| UNAUTHORIZED ABSENCES | |
| Unauthorized absence from a care provider facility or foster home | ORR SIR Triage Team elevates to the Field Manager, PO Supervisor, Division of UC Field Operations Director, Division of Grants Management Manager, ORR UC Bureau Chief, Deputy Assistant Secretary for Humanitarian Services, and ORR Director. |
| DEATH OF A CHILD, STAFF, OR OTHER PERSON IN A CARE PROVIDER FACILITY OR FOSTER HOME | |
| Death of a child | ORR SIR Triage Team elevates to the Field Manager, PO Supervisor, Division of UC Field Operations Director, Division of Grants Management Manager, ORR UC Bureau Chief, Deputy Assistant Secretary for Humanitarian Services, ORR Director, and DHUC Director. |
| Death of staff or other person | ORR SIR Triage Team elevates to the Field Manager, PO Supervisor, Division of UC Field Operations Director, Division of Grants Management Manager, ORR UC Bureau Chief, Deputy Assistant Secretary for Humanitarian Services, and ORR Director. |
| SITUATIONS IN WHICH THE LIVES OF CHILDREN OR CARE PROVIDER STAFF ARE IN IMMEDIATE DANGER | |
| Cases that affect the entire care provider facility | ORR SIR Triage Team elevates to the Field Manager, PO Supervisor, Division of UC Field Operations Director, Division of Grants Management Manager, ORR UC Bureau Chief, Deputy Assistant Secretary for Humanitarian Services, ORR Director, and DPL Director. |
| Medical emergency and mental health emergencies requiring hospitalization | ORR SIR Triage Team elevates to the Field Manager, PO Supervisor, Division of UC Field Operations Director, Division of Grants Management Manager, ORR UC Bureau Chief, Deputy Assistant Secretary for Humanitarian Services, ORR Director, and DHUC Director. |
| Potential infectious disease outbreak | – FFS Supervisor reports to DHUC. – DHUC reports confirmed outbreaks to the Field Manager, DPL Director, PO Supervisor, Division of UC Field Operations Director, Division of Grants Management Manager, ORR UC Bureau Chief, Deputy Assistant Secretary for Humanitarian Services, and ORR Director. |
Revised 08/01/2024
5.8.6 Allegations of Sexual Abuse in ORR Care
ORR has a zero-tolerance policy for sexual abuse, sexual harassment, inappropriate sexual behavior, and staff code of conduct violations at care provider facilities and foster homes, prioritizing a safe programmed care environment. See Section 4.10 Sexual Abuse Reporting and Follow-up for detailed reporting information.
Revised 6/7/2021
5.8.7 Allegations of Child Abuse in DHS Custody
If a UC alleges child abuse (including sexual abuse, sexual harassment, or inappropriate sexual behavior) in U.S. Department of Homeland Security (DHS) custody, care providers must report the allegation under state mandatory reporting laws and ORR policies/procedures. See definitions for physical abuse, verbal/emotional abuse, neglect, and medical neglect in the Guide to Terms. This ensures accountability across all stages of programmed care.
Care providers must document the allegation as a Historical Disclosure (Section 5.8.12 Behavioral Notes and Historical Disclosures) in ORR’s case management system within 24 hours. ORR then reports these abuse allegations to DHS Customs and Border Protection and DHS Office for Civil Rights and Civil Liberties.
Revised 6/7/2021
5.8.8 Reporting SIRs and Historical Disclosures to DHS
The chart below outlines care provider reporting requirements for significant incidents and historical disclosures that must be reported to DHS.
Care providers must not include clinical or mental health information in SIRs or historical disclosures reported to DHS unless required by mandatory reporting laws, maintaining appropriate programmed care confidentiality.
Quick Reference Chart: Care Provider Reporting Requirements for Significant Incidents and Historical Disclosures to DHS
Note: This chart is a quick reference and not exhaustive.
| TYPE OF INCIDENT | CARE PROVIDER REPORTING REQUIREMENTS |
|---|---|
| INCIDENTS THAT OCCURRED IN ORR CARE | |
| Unauthorized absence | 1. Report to 9-1-1 or local law enforcement, as appropriate. 2. Report to Child Protective Services (CPS) and/or State licensing officials and include the SIR Triage Team at [email protected]*. 3. Report to the ORR FFS Supervisor 4. Contact DHS’ Field Office Juvenile Coordinator (FOJC) by telephone. 5. Submit an Emergency SIR in ORR’s case management system within four (4) hours. 6. Submit an Emergency SIR to the FOJC within four (4) hours and include the SIR Triage Team at [email protected]*. Call the National Center for Missing and Exploited Children (NCMEC) Hotline at 1-800-THE-LOST (1-800-843-5678). |
| Arrest | 1. Submit an SIR in ORR’s case management system within four (4) hours. 2. Submit an SIR to the FOJC via email and include the SIR Triage Team at [email protected]*. Contact the FOJC by telephone. |
| Care Provider Facility Evacuations that result in the relocation of child to another facility | 1. Report to 9-1-1 or local law enforcement, as appropriate. 2. Report to CPS and/or State licensing officials and include the SIR Triage Team at [email protected]*. 3. Report to the ORR FFS Supervisor 4. Contact DHS’ Field Office Juvenile Coordinator (FOJC) by telephone. 5. Submit a Program-Level Event Report in ORR’s case management system within four (4) hours. Submit a Program-Level Event Report to the FOJC within four (4) hours and include the SIR Triage Team at [email protected]*. |
| INCIDENTS THAT DID NOT OCCUR IN ORR CARE | |
| Abuse (other than sexual abuse) or Neglect that Occurred in DHS Custody | 1. Report to CPS in the state of the reporting care provider, according to State mandatory reporting laws and include the SIR Triage Team at [email protected]*. 2. Report to CPS in the state where the allegation took place according to State mandatory reporting laws and include the SIR Triage Team at [email protected]*. 3. Submit historical disclosure in ORR’s case management system within 24 hours (ORR will provide a copy of the disclosure to the appropriate components of DHS). |
| Sexual Abuse, Sexual Harassment, or Inappropriate Sexual Behavior that Occurred in DHS Custody | Refer to the quick reference guide in Section 4.10.2 Care Provider Reporting Requirements. |
* Where notification occurs via email. For entities requiring website/portal notification, upload a copy of the completed form into ORR’s case management system as an SIR addendum.
The chart below outlines ORR/Federal Field Specialist (ORR/FFS) reporting requirements for significant incidents to DHS.
Quick Reference Chart: FFS Reporting Requirements for Significant Incidents to DHS
Note: This chart is a quick reference and not exhaustive.
| TYPE OF INCIDENT | FFS REPORTING REQUIREMENTS |
|---|---|
| Alleged or Suspected Human Smuggling, Drug Trafficking, and Weapons Trafficking | Email the SIR to the Immigration and Customs Enforcement (ICE)/Homeland Security Investigations (HSI) Tip Line within one business day of receiving the SIR. |
| Alleged or Suspected Human Trafficking | 1. Email the SIR to the ICE/HSI Tip Line within one business day of receiving the SIR. 2. Email the SIR to the ICE Human Trafficking Help Desk within one (1) business day of receiving the SIR. |
| Death of an Unaccompanied Child (See Section 3.3.16 Notification and Reporting of the Death of an Unaccompanied Child) | 1. Contact the child’s parent(s), legal guardian, or next-of-kin. 2. Contact the child’s attorney of record or the care provider’s local legal service provider. 3. Contact the applicable consulate officials. 4. Contact the child advocate, if applicable. 5. Contact the FOJC by telephone. 6. Contact the local medical examiner to obtain a death certificate. |
Revised 08/01/2024
5.8.9 Allegations of Past Abuse that Occurred Outside of the United States
If a UC reports past abuse outside the U.S. (home country or journey), care providers must document it as a Historical Disclosure (Section 5.8.12 Behavioral Notes and Historical Disclosures) and follow state licensing requirements to report abuse allegations, ensuring comprehensive programmed care documentation. Notification emails to external entities must include the Significant Incident Report (SIR) Triage Team at [email protected] for incident tracking and reporting compliance.
Revised 08/02/2023
5.8.10 Allegations of Past Abuse that Occurred Inside of the United States
All allegations of abuse within the U.S. (outside federal custody) must be reported to the care provider’s state licensing agency, Child Protective Services (CPS), and local law enforcement, under state licensing requirements, and documented as a Historical Disclosure (Section 5.8.12 Behavioral Notes and Historical Disclosures). For U.S. sexual abuse allegations, care providers must also elevate the case to the ORR Prevention of Sexual Abuse Coordinator at [email protected]. This ensures consistent programmed care response regardless of abuse location.
If state licensing or CPS agencies directly report allegations to law enforcement, care providers do not need to make separate reports but must confirm and document the report. Care providers must report adult-involved abuse allegations to local law enforcement, regardless of state licensing or CPS reporting. Notification emails to external entities must include the SIR Triage Team at [email protected] for incident tracking and reporting compliance.
Revised 08/02/2023
5.8.11 Notification to Attorneys, Legal Representatives, Child Advocates, Families, and Sponsors
Care providers must notify attorneys of record, legal service providers (LSP), child advocates, parents/legal guardians, and potential sponsors of specific Significant Incident Reports (SIRs), ensuring transparent programmed care communication.
Referrals/Notifications to Legal Service Providers and Attorneys of Record
Care providers MUST automatically refer children to on-site LSPs (or notify attorneys of record, if applicable) for legal screenings for:
- Emergency SIRs:
- Incidents Involving Weapons
- Severe Abuse/Neglect
- SIRs:
- External Threats to unaccompanied children
- Incidents Involving Law Enforcement On-Site
See also Section 4.10.4 Notification and Access to Attorneys/Legal Representatives, Families, Child Advocates, and Sponsors and Section 5.8.12 Behavioral Notes and Historical Disclosures for other circumstances requiring LSP/attorney referrals.
Care providers must explain to children that they are being automatically referred to attorneys to assess incident impacts on immigration cases, ensuring informed programmed care. Referrals must occur within 48 hours of care provider SIR awareness.
- For children 14 and older: Care providers must not disclose the SIR/Emergency SIR type requiring LSP/attorney referral.
- For children 13 and younger or with diagnosed developmental disabilities: Care providers must automatically disclose the SIR/Emergency SIR type (but not the SIR itself) in email referrals.
Care providers must not provide SIR copies (or related information) for legal screenings unless LSPs/attorneys complete Authorization for Release of Records under Section 5.10.1 UC Case File Request Process.
For UC Unauthorized Absences, care providers must also automatically notify LSPs/attorneys of record (if applicable) within 48 hours.
Referrals to Child Advocates
Care providers MUST automatically refer children to Child Advocates for:
- Emergency SIRs:
- Severe Abuse/Neglect
- SIRs:
- Incidents Involving Law Enforcement On-Site
- External Threats to unaccompanied children
Care providers must clarify automatic Child Advocate referrals (if not already appointed) to provide best-interest recommendations for UC care/placement, integral to holistic programmed care. Referrals must occur within 48 hours of care provider SIR awareness.
Care providers must use the Child Advocate Recommendation and Appointment Form (ORR case management system) for referrals.
Care providers may only provide complete case files (including SIR documentation) to Child Advocates after confirmation of appointment and receipt of completed Child Advocate Recommendation and Appointment Forms.
For UC Unauthorized Absences, care providers must automatically notify appointed Child Advocates (if any) within 48 hours.
For UCs hospitalized or requiring serious medical services, care providers must notify child advocates (if applicable), parents/legal guardians, and sponsors (see Section 4.10.4 Notification and Access to Attorneys/Legal Representatives, Families, Child Advocates, and Sponsors and Figure 4.10.2).
More Child Advocate role information is in Section 2.3.4 Child Advocates.
Arrests
Care providers should prioritize de-escalating conflicts to prevent law enforcement contact (see Section 3.3.13 Behavior Management).
If a UC is arrested, care providers should—within four (4) hours of arrest during business hours or the next morning—notify:
- UC parent/legal guardian, if possible and no child welfare reasons prohibit notice.
- LSP or attorney of record (if applicable).
- Appointed Child Advocate (if applicable).
- Potential sponsor, if possible and no child welfare reasons prohibit notice.
Notifications must specify:
- UC arrest, but:
- For children 14 and older: care providers must not disclose arrest details unless the child consents.
- For children 13 and younger or with diagnosed developmental disabilities: care providers must automatically disclose known arrest details.
- UC present location (if known).
- Law enforcement point of contact.
- Public defender point of contact (if known).
Care providers must make timely and reasonable efforts to notify law enforcement of information ensuring immediate UC safety in custody (current medications, allergies, disability-related needs, suicide risk). This is part of responsible programmed care coordination.
ORR will plan for UC return to ORR custody within one calendar day of arrest to ensure appropriate placement availability upon release and minimize post-release wait times.
Notification and Access to Families and Sponsors
Care providers must notify parents/legal guardians and potential sponsors of abuse/neglect, on-site law enforcement incidents, and unauthorized absences, ensuring family engagement in programmed care. Facilities must ensure UC family access (including legal guardians), unless ORR has documented safety concerns. Only notifications are required, SIRs are not sent.
If a UC is arrested, care providers should—within four (4) hours of arrest during business hours or the next morning—notify UC parents, legal guardians, and/or sponsors, if possible and no child welfare reasons prohibit notice.
Quick Reference Chart: Notification to Parents/Legal Guardians and Sponsors
| CHILD’S AGE | CARE PROVIDER REQUIREMENTS |
|---|---|
| 14 Years Old or Older | 1. Follow child’s decision on parent/legal guardian notification unless evidence indicates non-notification. 2. Follow child’s decision on sponsor/receiving facility notification (if different from parent/legal guardian). |
| 14 Years of Age or Older with a Diagnosed Developmental Disability | Notify ORR/FFS before speaking with the child. |
| 13 Years of Age or Younger | 1. Notify UC parent/legal guardian unless evidence indicates non-notification. 2. Notify UC sponsor/receiving facility (if different from parent/legal guardian). |
Care providers must document all notifications in ORR’s case management system.
Revised 08/02/2023
5.8.12 Behavioral Notes and Historical Disclosures
Behavioral Notes
Care providers may document UC behaviors or observations highlighting positive events/developments or patterns meriting intervention (life skill improvement, class performance, benign horseplay, adolescent non-compliance), adding context to UC time in ORR care and informing support/relevant services, enhancing individualized programmed care. Behavioral Note documentation is optional at care provider discretion.
Care providers must never threaten UCs with Behavioral Note use for behavior control.
Behavioral Notes are subject to information sharing prohibitions in Section 5.10.2 Limits to Sharing Information with DHS and EOIR (ORR prohibits non-essential case information sharing with DHS/EOIR, including behavioral reports). ORR will not release records to government agencies if requests are outside agency authority or appear to be for immigration enforcement (even with authorization) without lawful subpoenas/court orders (see Section 5.10.1 UC Case File Request Process). Behavioral Notes are also subject to information sharing prohibitions in Section 5.9.2 Protecting Confidentiality of Mental Health and Medical Records and Disclosure Notice Requirements in Section 5.9.1 Requirement to Inform Children of Limits to Confidentiality.
Historical Disclosures
Incidents predating ORR care should be documented as Historical Disclosures (Section 5.8.12 Behavioral Notes and Historical Disclosures) in ORR’s case management system within 24 hours of UC disclosure. Examples include DHS custody abuse/neglect, U.S. abuse/neglect outside federal custody, or home country trauma. Historical Disclosures document past abuse, neglect, harm, or threats prior to ORR care to inform best care approaches, such as mental health support. Documentation also helps notify investigative entities of threats like human trafficking. Care providers are responsible for relevant support services in response to historical disclosures (mental health support following trauma disclosure), a key aspect of trauma-informed programmed care.
Reporting Requirements
Care providers must report past abuse/neglect in home countries, journeys, or U.S. prior to ORR care to relevant state child protective service entities, state licensing, and/or law enforcement, as appropriate, under mandatory reporting laws, state licensing requirements, federal laws/regulations, and ORR policies/procedures within 24 hours of disclosure.
Care providers must also report certain disclosures to other stakeholders, as outlined below.
See also Section 4.10.4 Notification and Access to Attorneys/Legal Representatives, Families, Child Advocates, and Sponsors and Section 5.8.11 Notification to Attorneys, Legal Representatives, Child Advocates, Families, and Sponsors for additional LSP/Child Advocate referral requirements.
Referrals/Notifications to LSPs and Attorneys of Record
Care providers must automatically refer children to legal service providers (LSPs) (or notify attorneys of record, if applicable) for legal screenings within 48 hours for the following Historical Disclosures:
- Abuse/Neglect in DHS Custody
- Past Abuse/Neglect Not in ORR or DHS Custody
- Self-Disclosed Juvenile Delinquency
Care providers must explain to children that automatic attorney referrals are for assessing disclosure impacts on immigration cases, ensuring informed programmed care.
- For children 14 and older: Care providers must not disclose the historical disclosure type requiring LSP/attorney referral.
- For children 13 and younger or with developmental disabilities: Care providers must automatically disclose the historical disclosure type (but not the disclosure itself) in email referrals.
Care providers must not provide Historical Disclosure copies for legal screenings unless LSPs/attorneys complete Authorization for Release of Records under Section 5.10.1 UC Case File Request Process.
Referrals to Child Advocates
Care providers must automatically refer children to Child Advocates within 48 hours for the following Historical Disclosures:
- Labor Trafficking
- Sex Trafficking
Care providers must clarify automatic Child Advocate referrals (if not already appointed) to provide best-interest recommendations for UC care/placement, ensuring holistic programmed care.
Care providers must use the Child Advocate Recommendation and Appointment Form (ORR case management system) for referrals, providing basic referral reason information.
Care providers may only provide complete case files (including SIR/Historical Disclosure documentation) to Child Advocates after appointment confirmation.
More Child Advocate role information is in Section 2.3.4 Child Advocates.
Reporting Sexual Abuse and Sexual Harassment that Occurred in DHS Custody
For DHS custody sexual abuse, sexual harassment, and inappropriate sexual behavior allegations, care providers must follow reporting requirements in Section 5.8.8 Reporting SIRs and Historical Disclosures to DHS, reporting within 24 hours. Suspicions of human trafficking/smuggling must be reported to the Office of Trafficking in Persons (OTIP) within 24 hours. Other sexual abuse, harassment, and inappropriate behavior allegations outside ORR/DHS custody should be reported under Section 4.10.2 Care Provider Reporting Requirements.
Note: Only some Historical Disclosure notes are DHS-reportable (listed in Section 5.8.8). Other disclosures within Historical Disclosures not listed in Section 5.8.8 cannot be shared with DHS without (1) UC consent and (2) case file request process completion (see Section 5.10.1 UC Case File Request Process, and must comply with Section 5.10.2, Limits to Sharing Information with DHS and EOIR).
For health-related historical disclosures, care providers will also notify ORR’s Division of Health for Unaccompanied Children, ensuring integrated programmed care.
Posted 08/02/2023
5.9 Protecting the Privacy and Confidentiality of Unaccompanied Alien Children Information
The following sections outline ORR internal agency policies and practices for protecting UC information privacy and confidentiality and limits to confidentiality for certain information shared by UCs in ORR care. ORR treats information in ORR systems of records on non-U.S. persons, including UC and sponsor case files, as subject to Privacy Act administrative provisions, ensuring rigorous programmed care data protection.
UC Bureau records include all records pertaining to individual UCs and former UCs, including all information collected by care providers or ORR staff (written and electronic), including records in Section 5.6.2 Maintaining Case Files 9. All UC Bureau contractors and grantees must comply with Privacy Act requirements when accessing or using Department Privacy Act-protected records.
As stated in Section 5.3.3 Prohibition on Release of Records Without Prior Approval, UC Bureau records are ORR property and cannot be released without prior ORR approval per ORR UC Bureau Policy Guide policies. UC Bureau records contain highly sensitive program participant information and must be kept confidential and protected from unauthorized disclosure for privacy and safety reasons.10 However, ORR/HHS may need to provide UC case file information in lawsuits or UC Bureau oversight investigations, audits, evaluations, and inspections by the HHS Office of the Inspector General (OIG), Government Accountability Office (GAO), or Congressional inquiries (see Section 5.10.7 Information Sharing with Investigative Agencies for child safety/case file investigation requirements).
The sections below describe ORR records privacy/confidentiality policies/practices for UC Bureau records and record request procedures.
Revised 08/07/2023; Effective 08/21/2023
5.9.1 Requirement to Inform Children of Limits to Confidentiality
ORR ensures children are informed of confidentiality limits for information shared in ORR care, including information types and entities to which care providers and ORR must disclose information for UC or other safety. Care providers must verbally explain the Disclosure Notice to each child in their preferred language twice—once before UC Assessment completion and again before clinical sessions, as noted in Section 3.2.1 Admissions for Unaccompanied Children. The Disclosure Notice must be reviewed again with children after each ORR network transfer, following the same timeframe requirements (pre-UC Assessment and pre-clinical sessions). This is a standard practice in programmed care.
The Disclosure Notice explains that most information disclosed in counseling or assessments remains confidential, but confidentiality exceptions exist for UC or other safety, under mandatory reporting requirements and Section 5.8 Reporting Child-Level and Program-Level Events. UCs are also informed that mental health information is not released to DHS without consent.
Care providers must inform UCs of situations where case files/records may be shared with outside entities in limited scenarios (federal court subpoenas). Care providers must have accountability systems and policies to protect UC information and record confidentiality from unauthorized use/disclosure, adhering to:
Revised 08/01/2024
5.9.2 Protecting Confidentiality of Mental Health and Medical Records
Recognizing the confidential nature of clinical sessions, most information disclosed by UCs during sessions in ORR care, and related documentation (therapist/clinician case notes/records), remains confidential and is only released under policies in this section and Section 5.10 Information Sharing11. ORR also does not share clinical/mental health records with immigration courts for master calendar hearings not involving UC custody decisions (see Section 5.10.2 Limits to Sharing Information with DHS and EOIR).12 This protects the privacy integral to effective programmed care.
When ORR requires UC consent to share mental/medical health records, but UCs in ORR custody are unable to consent due to age, diagnosed developmental disabilities, or other medical/mental health conditions, ORR generally provides consent when information is needed for service provision under Section 3.3 Care Provider Required Services.
For medical record confidentiality policies related to pregnancy, birth, and abortion, see the Policy Memorandum: Medical Services Requiring Heightened ORR Involvement (PDF).
If medical/mental health records are requested for reasons other than service provision, ORR requires authorizing signatures and consent from the UC or caregiver (parent/legal guardian/sponsor) as specified in Figure 5.10.3 Signature Requirements for Release of Sensitive Information. If released UCs are unable to consent due to age, disability, or condition, ORR requires caregiver (parent/legal guardian/sponsor) consent. If caregivers cannot provide consent (orphaned UCs, unlocatable parents), ORR may consent to medical/mental health record release if in the UC’s best interests. Care providers must also follow applicable state laws regarding medical/mental health record release consent.
If local law enforcement or investigative agencies request medical records through the case file request process for UCs missing from ORR care or post-release, records may only be shared with UC Bureau Director approval.
Revised 08/07/2023; Effective 08/21/2023
5.10 Information Sharing
The following sections detail ORR internal policies/practices for protecting privacy when sharing information, procedures for requesting ORR information (case files), and information ORR does/does not share with government/law enforcement agencies and stakeholders, ensuring responsible programmed care data handling. These policies do not apply to Child Advocates, who have full client case file access and can request copies directly from care providers without standard ORR processes, as per Section 5.10.3 Information Sharing with LSPs, Attorneys of Record, and Child Advocates.
Subject to whistleblower protection laws, care provider facility or Post-Release Services (PRS) provider employees, former employees, or contractors must not disclose UC case file records or information about UCs, sponsors, families, or household members to anyone for any purpose (except program administration) without prior ORR notice, allowing ORR to ensure UC information disclosure is compatible with program goals and UC safety/privacy. Some UC information is intensely personal (Child-Level Events, abuse allegations, mental health/suicidal ideation documents, pregnancy termination documents, trauma recounts). ORR will evaluate if available information, including event recitations, could identify report subjects. Considering ORR’s directive under 8 U.S.C. § 1232(c)(1) to protect UCs from exploitation, including witness protection program policies, and the responsibility to consider UC interests in care/custody decisions under 6 U.S.C. 279(b)(1)(B), and the intensely personal nature of juvenile information, ORR may deny requests if information should be protected, even if policy permits record requests and disclosure.
ORR is not an immigration enforcement agency and does not share information with DHS, DOJ, or similar entities for immigration enforcement.
ORR, as UC information custodian, may use UC case file information for its operations, prosecution, and defense. ORR may provide UC information outside the case file request process in response to UC Bureau oversight audits, evaluations, investigations, and inspections by HHS Office of the Inspector General (OIG) or Government Accountability Office (GAO) or Congressional inquiries (see Section 5.10.7 Information Sharing with Investigative Agencies for child safety/case file investigation requirements). For information sharing with litigants adverse to HHS, ACF, and/or ORR, UC Bureau contractors and grantees must adhere to federal civil procedure rules, including responding to discovery orders in federal litigation. Care providers must take steps to protect record confidentiality in litigation by seeking court protective orders. These policies do not apply to Freedom of Information Act (FOIA) requests, which are subject to Department-wide rules.
Revised 08/01/2024
5.10.1 UAC Case File Request Process
As stated in Section 5.3.3 Prohibition on Release of Records Without Prior Approval, UC Bureau records are ORR property and cannot be released without prior ORR approval. Requests for UC and/or released UC case file records must be made directly to ORR, not to the Administration for Children and Families (ACF) Freedom of Information Act (FOIA) office, ensuring streamlined programmed care information access.
ORR works closely with stakeholders to ensure UC safety and well-being. Certain stakeholders may request case file records (see Section 5.6.2 Maintaining Case Files for typical case file records). Stakeholders include ORR-funded legal service providers (LSPs), attorneys of record, child advocates, released children, sponsors/potential sponsors, UC parents/legal guardians, educational institutions/medical providers serving UCs post-release, and other federal/state government agencies. ORR protects the safety and privacy of UCs, sponsors/potential sponsors, household members, foster parents, and others whose information ORR holds when processing requests.
Revised 08/07/2023; Effective 08/21/2023
5.10.1.1 Authorization for Release of Records Form
All requesters (except child advocates, see Section 5.10.3 Information Sharing with LSPs, Attorneys of Record, and Child Advocates) must complete the Authorization for Release of Records (ARR) (PDF) form and submit it with required supporting documentation to [email protected] for ORR pre-approval. ORR, at its discretion, may reject requests for incomplete forms, non-compliance with policies, safety reasons, or other reasons, considering the UC’s best interests. ARR forms do not cover medical service record requests for UCs in care (see Section 3.4.3 Requests for Health Care Services and Section 3.4.7 Maintaining Health Care Records and Confidentiality). This process ensures controlled programmed care information access.
Verifying Identity of Requestor
ORR verifies requester identity and legitimate reasons for case file record requests when reviewing ARR forms. Some requesters must provide supporting documentation. The table below outlines supporting documentation requirements by requester type. ORR may request additional documentation as needed.
Figure 5.10.1: Required Supporting Documentation
The table below outlines supporting documentation requirements by requestor type for UC case files:
| TYPE OF REQUESTER | SUPPORTING DOCUMENTATION |
|---|---|
| Attorney or Board of Immigration Appeals (BIA) accredited representative representing the child before an immigration court | Notice of Attorney Representation |
| Attorney representing the child in an ORR bond hearing or other individual matter related to transfer to a restrictive placement or release from ORR custody | Notice of Attorney Representation |
| Attorney representing the child on other individual matters | Notice of Attorney Representation |
| ORR-funded legal service providers conducting a legal screening pursuant to Section 3.7.1 Know Your Rights Presentation & Screenings for Legal Relief | Notice of Attorney Representation |
| Representative of a Federal/State government agency (e.g., DHS, EOIR, HHS/OIG, state police departments, GAO, Child Protective Services, State Licensing) or the National Center for Missing or Exploited Children | A statement on the agency’s official letterhead verifying the requesting party’s affiliation, specifies the scope of their investigation, and includes a case reference number, investigation number or warrant to indicate jurisdiction over a case. OR A lawfully-issued subpoena or court order |
| Current unaccompanied child | None |
| Former unaccompanied child | ORR Verification of Release form or government-issued photo identification (see Section 2.2.4 Required Documents for Submission with the Application for Release for a list of acceptable proof of identity documents) |
| Sponsor or parent/legal guardian13 | Government-issued photo identification (see Section 2.2.4 for a list of acceptable proof of identity documents). |
| Educational institution or medical provider | A statement on the organization’s official letterhead verifying that the requesting party is providing educational or medical services to the subject of the record request |
Revised 08/07/2023; Effective 08/21/2023
5.10.1.2 Obtaining Authorization from the Subject of the Request
Requesters must obtain authorization from record request subjects (UC and/or sponsor) on the Authorization for Release of Records (ARR) (PDF) form before ORR record release. Authorization is evidenced by the subject and witness signatures. For example, ORR requires signatures from children 14 and older before information release. Similarly, sponsor/potential sponsor signatures are required for their information release, maintaining ethical programmed care data management.
ORR may deny record requests in part or whole if signature requirements below are not met.
Signature Requirements for Release of UC Case File Information
The following table describes ORR’s signature requirements for releasing UC information, based on UC age and ORR custody status.
Figure 5.10.2: Signature Requirements for Release of Unaccompanied Child Information
| IS THE CHILD IN ORR CUSTODY? | CHILD’S AGE | SIGNATURE REQUIREMENTS |
|---|---|---|
| Yes | 14 Years Old or Older | Child and a witness |
| 14 Years Old or Older with a Diagnosed Developmental Disability.14 OR Under 14 Years Old.15 | None. ORR may release information in its discretion in the best interests of the child.16 | |
| No | 14 Years Old or Older | Child and a witness |
| 14 Years Old or Older with a Diagnosed Developmental Disability OR Under 14 Years Old | Child’s caregiver (typically the sponsor) or parent/legal guardian, and a witness Note: If the child’s caregiver refuses to sign, ORR will release case file information at its discretion if the child’s caregiver is the subject of a legal proceeding related to their care of the child. |
In addition to the above, ORR specifically requires the following signatures for releasing particularly sensitive records.
Figure 5.10.3: Signature Requirements for Release of Sensitive Information
| RECORD CATEGORY | SIGNATURE REQUIREMENT |
|---|---|
| Medical Records | Child, the child’s caregiver (typically the sponsor), or the child’s parent/legal guardian |
| Clinical/Mental Health Services | Child, the child’s caregiver (typically the sponsor), or the child’s parent/legal guardian |
| Home Study Reports or Post-Release Services Records | Sponsor or potential sponsor |
Sponsor/potential sponsor signatures are required for home study reports and post-release service records. If sponsor signatures are not provided, ORR redacts all sponsor/potential sponsor/household member information from other UC case file records.
Signature Requirements for Requests from Government Agencies
ORR prefers government agencies to obtain subject authorizing signatures as outlined above. However, ORR may release limited record categories to government agencies without authorizing signatures at its discretion:
- Child information (name, A number)
- Child photograph (only without child consent when consent is unobtainable, photo provision is not for immigration enforcement, ORR determines provision is in UC best interests, and there is a legitimate child welfare reason (missing child cases). DHS/EOIR photo sharing limits are in Section 5.10.2 Limits to Sharing Information with DHS and EOIR).
- Placement documents
- Legal information (child legal representative name/contact information only)
- Educational services
- Case management records (telephone/visitor logs only)
- Discharge/release information:
- Verification of Release form
- Discharge Notification form
- Notice of Transfer to ICE Chief Counsel — Change of Address/Change of Venue form (if applicable)
- Copy of the Trafficking Eligibility Letter (if applicable)
- Basic Post-18 plan information (name, relationship, address, Post-18 plan individual)
ORR will not release UC or sponsor records to government agencies if requests are outside agency authority or appear to be for immigration enforcement (even with authorizing signatures) without lawful subpoenas17 or court orders, maintaining stringent programmed care data protection.
Revised 08/07/2023; Effective 08/21/2023
5.10.1.3 Case File Information that is Restricted from Release
ORR restricts release of certain UC case file information to the public or through case file requests that could pose safety risks or violate current/former UC privacy. In such cases (public release or case file requests), ORR does not release sponsor, potential sponsor, or household member information without their written consent. ORR may also redact law enforcement-sensitive information and information protected by privacy considerations, ensuring responsible programmed care data handling. ORR will not release the following information categories through case file requests unless required by lawful court subpoenas, orders, litigation, or federal investigation:
- Internal communications (care provider staff or ORR memoranda/emails to the extent they are in case files; not all emails/memoranda are considered case file information).
- Internal care provider incident reports.
- Sponsor Assessments.
- Family Reunification Packets.
- Background check results.
- Foster parent information.
- Information on other children not subject to information requests, unless siblings of the child whose information is requested.
Revised 08/07/2023; Effective 08/21/2023
5.10.1.4 Child’s Request for their Own Case File
UCs in ORR custody may request their own case file copies from ORR, using the Authorization for Release of Records (ARR) (PDF) form or requesting care provider assistance. Before providing case files, ORR redacts personal information of others (e.g., other UCs) to prevent unauthorized information disclosure, reinforcing programmed care privacy protections. Other parties cannot directly retrieve case file copies from UCs and must use the case file request process.
Revised 08/07/2023; Effective 08/21/2023
5.10.1.5 Timeframe for Processing Requests for UC Case File Documents
ORR processes case file requests in order of receipt. Generally, ORR fulfills requests within 40 calendar days of complete request receipt, ensuring reasonably timely programmed care information access. However, ORR may be unable to meet this timeframe if request volumes exceed 150 in a two-week period or for documents created before January 2014. In these cases, ORR informs requesters and fulfills requests as expeditiously as possible, considering receipt order and urgency.
Expedited processing may be requested for urgent situations requiring documents sooner than 40 calendar days.
ORR may expedite records requests within seven (7) calendar days for:
- UCs or released UCs reported missing to the National Call Center, National Center for Missing and Exploited Children, or investigative agencies with jurisdiction over missing UC cases (see Section 5.10.6 Information Sharing for Cases Involving Children Reported Missing).
- UCs with court hearings within 30 calendar days.
- UCs turning 18 in under 30 calendar days.
- UCs with risk determination hearings within 30 calendar days (see Section 2.9 Risk Determination Hearings).
- Records needed for UC medical services.
- Records needed for UC school enrollment/continued enrollment.
- Records requested for federal/state/local agency investigations (OIG, GAO, State licensing/CPS, law enforcement not related to immigration enforcement) (see Section 5.10.7 Information Sharing with Investigative Agencies).
- Any other situation where ORR deems expedited response warranted at its discretion.
ORR must provide attorneys of record and DOJ Accredited Representatives with key UC case file documents within seven (7) calendar days of properly submitted expedited record requests.
ORR may provide other requester types with key UC case file documents within seven (7) calendar days of properly submitted expedited requests.
ORR will prioritize investigation-related record requests for faster-than-seven-day processing to the extent possible. Requesters seeking expedited processing for other reasons may be approved at ORR discretion after considering requestor explanations for expedited processing necessity.
Key documents eligible for expedited processing:
- UC Assessment
- UC Case Review (two most recent)
- Assessment for Risk
- Referral information
- Initial Intakes Assessment
- Notice of Placement in a Restrictive Setting (if any for current placement)
- Completed Transfer Requests (if any for current/prior placement) or Verification of Release
- Potential sponsor contact information and Home Study Report (with potential sponsor approval)
- Individual Service Plan
- Child-Level Events (SIRs and Historical Disclosures only) for current placement (for >10 Child-Level Events, attorneys should specify requested event types for expedited processing)
- UC identity documents (birth certificate)
- Medical and psychological examination reports (if any)
- Prescribed medication logs and consent forms
- Trafficking eligibility letter copy (if any)
- Notice to Appear.
Revised 08/01/2024
5.10.2 Limits to Sharing Information with DHS and EOIR
House Report 116-450 (PDF), accompanying the Consolidated Appropriations Act, 2021 (PDF), directs ORR to restrict sharing specific case information with the Executive Office for Immigration Review (EOIR) and DHS that may dissuade UCs from seeking legal relief or bias courts and unfairly influence continuance issuances. ORR establishes the following policies per H.R. 116-450, ensuring ethical programmed care legal support.
Prohibition on Sharing Mental Health Information with DHS and EOIR
Per House Report 116-450 at 185, ORR does not transmit the following case file information types to ICE, CBP, or other DHS entities for immigration enforcement or to EOIR for immigration court use (removal proceedings, asylum determinations), unless ORR/care providers are parties/counsel in proceedings:
- Any mental health records or information from UC clinical mental health sessions.
- Any mental health information from UC or parent/legal guardian joint mental health sessions.
- Any mental health information from UC separate sessions to facilitate joint mental health sessions.
Prohibition on Sharing Non-Essential Case File Information with DHS and EOIR
Per House Report 116-450 at 184, ORR does not transmit non-essential case file information to EOIR/DHS when understood to be for immigration proceedings/enforcement. Neither ORR nor care providers are parties in immigration proceedings, upholding ethical programmed care principles.
Non-essential information examples include:
- Medical or mental health records and behavioral reports.
- UC immigration relief eligibility assessments.
- Potential sponsor immigration status information.
Limits on Sharing Biographic Information with DHS and EOIR
UC biographic information sharing with DHS/EOIR is limited to ORR UC service provisions and statutory authority under 8 U.S.C. 1232(b)(4) .
ORR may share UC biographic information (birth certificates, photographs) with DHS/EOIR in limited scenarios:
- Providing age determination evidence to DHS (see Section 1.6.2 Instructions).
- Correcting UC biographic information in government databases (ORR case management, Notice to Appear (NTA), etc.) when in UC best interests.
- Validating UC-separated parent/legal guardian relationships.
- Submitting Discharge Notifications to DHS.
- Submitting Case Status Summaries for EOIR pre-immigration hearings18.
- Facilitating sponsor participation in Legal Orientation Programs for Custodians (LOPCs) at EOIR under William Wilberforce Trafficking Victims Protection Reauthorization Act of 2008 section 235(c)(4), 8 U.S.C. 1232(c)(4).
- Providing Notice of Transfer to the Immigration and Customs Enforcement Chief Counsel Change of Address/Change of Venue, ORR Notification to ICE Chief Counsel Release of Unaccompanied Child to Sponsor and Request to Change Address, and Discharge Notifications to immigration courts.
- Providing information in response to court orders for legal proceedings where ORR/care providers are parties.
ORR may provide UC photographs to DHS for missing UC cases or child safety (trafficking) investigations, provided photos are not used for immigration enforcement. ORR must seek UC consent for photo release if possible but may release photos without consent if unobtainable and ORR determines release is in UC best interests (see also Section 5.10.1.2 Obtaining Authorization from the Subject of the Request).
FFS approval is required for UC biographic information provision to DHS/EOIR in these scenarios. UC attorneys of record or LSPs and Child Advocates (if applicable) are notified when UC biographic information is provided to DHS/EOIR and can address the matter directly with DHS/EOIR, ensuring transparency and legal oversight in programmed care.
Revised 08/07/2023; Effective 08/21/2023
5.10.3 Information Sharing with LSPs, Attorneys of Record, and Child Advocates
Information Provided for Know Your Rights (KYRs) and Legal Screenings
ORR shares limited information categories with legal service providers (LSPs) responsible for Know Your Rights (KYR) presentations and legal screenings, other LSPs, and attorneys of record, facilitating effective programmed care legal support.
ORR is authorized to provide basic information for LSPs conducting KYR presentations and legal screenings without the case file request process in Section 5.10.1 UC Case File Request Process. This information includes:
- UC census at LSP-assigned care providers.
- UC birth certificates (if available).
- Notice to Appear (NTA, DHS Form I-862) (if available).
- Report of a Deportable/Inadmissible Alien (DHS Form I-213) (if available).
- Arrival/Departure Record (DHS Form I-94) (if available/applicable).
- Documents UCs bring (if UC grants permission).
- UC family member contact information (if UC grants permission) (e.g., family phone numbers)19.
- Information on UC siblings in ORR care and their care provider placements (if applicable).
- Notification of UC family separation (if applicable).
- Notification of UC removal orders (if applicable), including Migrant Protection Protocols (MPP) removal orders20.
ORR will provide DHS-issued forms about UCs to LSPs for legal screenings if DHS has previously provided them to ORR. ORR cannot provide DHS-issued forms not in its possession.
In rare necessary cases, ORR may provide additional LSP information for legal screenings after LSPs follow the case file request process in Section 5.10.1 UC Case File Request Process.
Case Management Updates to Stakeholders
Per Section 2.3.2 Case Managers, care providers must provide weekly case management decision updates to stakeholders (LSP, attorney of record, Child Advocate if assigned). Care providers must notify stakeholders of final release decisions, UC aging out/leaving care, sponsorship changes, no viable sponsors (Category 4 cases), UC transfer recommendations/initiations (long-term foster care or other care levels), and approved UC transfers, ensuring stakeholder awareness in programmed care. These updates inform LSPs, attorneys, and Child Advocates of UC case progress, which may impact immigration cases and legal relief eligibility. LSPs, attorneys, and Child Advocates can make recommendations but are not ORR sponsor assessment or release decision-makers.
Care providers should also provide case status updates to stakeholders pre-immigration hearings and as part of weekly census updates. Case managers should share information permitted for immigration court sharing on Case Status Summary Forms for EOIR pre-immigration hearings (see Section 5.10.2 Limits to Sharing Information with DHS and EOIR). This information includes:
- UC Name (and alias if applicable)
- A Number
- Date Entered ORR Care
- Days in ORR care (length of stay and care)
- Sponsor Category
- Program/Facility Name and Address
Child Advocates are permitted to attend case staffings between FFS, case managers, and case coordinators regarding UC placement/release assessments and have access to complete case files per Section 2.3.4 Child Advocates.
LSPs and attorneys of record are not permitted to attend case staffings between FFS, case managers, and case coordinators regarding UC family reunification assessments. However, case managers must provide weekly case management decision/progress updates to LSPs/attorneys as outlined above (see Section 2.3.2). LSPs/attorneys are encouraged to seek UC permission to share legal case updates with case managers for coordinated case management and legal services. LSPs must enter representation for Category 4 UCs, UCs in long-term foster care, and UCs in the URM program. Weekly updates to LSPs on UC likelihood of meeting mandatory representation categories are important for LSP contractual obligation fulfillment. Further information requests from LSPs/attorneys about UC cases should follow the case file request process in Section 5.10.1.
Notification of Transfers and Discharges to Stakeholders
ORR will notify LSPs, attorneys of record, and Child Advocates (if appointed) of UC transfer recommendations/initiations to other facilities (including out-of-network placements, see Section 1.4 Transfers within the ORR Care Provider Network ) and UC discharge from ORR custody (see Section 2.8 Release from Office of Refugee Resettlement (ORR) Custody), ensuring stakeholder involvement in UC programmed care transitions.
Requests for Case File Information from LSPs and Attorneys of Record
For other case file information categories, LSPs/attorneys of record generally must follow the process in Section 5.10.1, including Notice of Attorney Representation (PDF) submission, to request specific UC case file information. See Section 3.7.3 Attorney Request for Information on UC Case for shareable information. This section does not limit LSP access to information under Section 4.10.4 Notification and Access to Attorneys/Legal Representatives Families, Child Advocates, and Sponsors, Section 5.8 Reporting Emergencies, Significant Incidents, and Program-Level Events, or other ORR policies/guidance/procedure notices to LSPs.
Child Advocates’ Access to Case File Information
Child Advocates have access to complete UC case files per Section 2.3.4 Child Advocates. Upon presenting Child Advocate Recommendation and Appointment forms as assignment proof, they may request and receive case file documents directly from ORR care providers. Child Advocates must keep case file information and UC case details confidential from non-ORR grantees, contractors, and federal staff, ensuring UC privacy within programmed care.
Revised 08/07/2023; Effective 08/21/2023
5.10.4 Information Sharing Agreements for Child Welfare Purposes
ORR may enter agreements with state/local governments and child welfare agencies (National Center for Missing and Exploited Children) to share general UC Bureau information or aggregated/de-identified UC information, considering UC safety concerns or direct service provision during ORR care or post-release, independent of the case file request process in Section 5.10.1 UC Case File Request Process. ORR will consider information sharing agreement requests with state/local governments and child welfare agencies, considering UC best interests and ORR administrative burden, ensuring responsible programmed care data collaboration. Information sharing agreements must not be for immigration enforcement.
ORR may also enter written data sharing agreements to disclose UC and sponsor biographic information in limited circumstances to state/local child welfare agencies or agencies offering services benefiting UCs in care/post-release or sponsors, if ORR determines information provision is in UC best interests; no confidential/privileged information is disclosed without UC/sponsor consent; valid child welfare interest exists in ORR discretion for sharing information; information release does not impose undue ORR administrative burden; and information is not used for immigration enforcement or shared with law enforcement for non-child welfare purposes. Prior to information disclosure, ORR must enter written agreements with state/local governments or child welfare agencies outlining authorized information use.
Revised 08/07/2023; Effective 08/21/2023
5.10.5 Information Sharing on Separated Children
This section describes ORR information sharing requirements with Congress, DHS, and other stakeholders regarding children separated from parents/legal guardians under the “Zero Tolerance” immigration policy (no longer in effect)21, ensuring transparency in programmed care for separated families.
Mandatory Notification
For as long as necessary to fulfill applicable court orders, settlements, or legal requirements related to child separations and family reunifications, and per House Report 116-450 at 186, ORR will promptly notify legal service providers (LSPs) assigned to UC programs and UC attorneys of record upon learning UCs may have been separated from parents/legal guardians by DHS or processed under Migrant Protection Protocols (MPP). ORR also reports monthly to Congress on UC numbers in care separated from parents/legal guardians by DHS, per the Consolidated Appropriations Act, 2024 and House Report 116-450 (PDF).
When required, ORR/care providers will provide LSPs assigned to UC programs and UC attorneys of record with available ORR information on separated UC family members, including locations and contact information, and will facilitate routine UC-family communication. ORR also seeks information from DHS to determine separation reasons and separated parent/legal guardian locations, facilitating family reunification within programmed care.
Communication with LSPs, Attorneys of Record, and Child Advocates
To obtain additional separation case information, LSPs/attorneys of record with Notice of Attorney Representation (Form L-3) (PDF) must submit case file record requests under Section 5.10.1 UC Case File Request Process. Child Advocates have full UC case file access and may make written requests via email to UC care providers, copying ORR FFS, for additional information on DHS border-separated families. Additional information requests from LSPs, attorneys, and Child Advocates must identify the UC, specify needed information, and state request reasons. In stating reasons, LSPs must describe request relation to ORR legal services contracts or child advocacy. ORR will not authorize information release to LSPs for reasons unrelated to legal services contracts or without Notice of Attorney Representation. ORR provides initial responses to information requests within seven days. LSP and attorney of record separated UC case file information requests must follow Section 5.10.1 policy. Information sharing with Child Advocates follows policies in Section 5.10.3 Information Sharing with LSPs, Attorneys of Record, and Child Advocates and Section 2.3.4 Child Advocates.
Birth Certificate Authentication and DNA Testing
In rare cases, ORR may authorize birth certificate authentication or DNA testing of separated parents and children to validate relationships, supporting family reunification within programmed care. Parent/legal guardian DNA submission is voluntary and requires consent. Children 14 and older without developmental disabilities must voluntarily consent to DNA submissions. ORR will provide consent for children under 14 for relationship-establishing DNA submissions. For children 14 and older with developmental disabilities, FFS consultation is needed for best interest determinations on UC consent. Case Managers must provide advance notice to UC attorneys of record/LSPs of DNA testing. If positive relationship proof is obtained, ORR notifies DHS of confirmed separations. ORR destroys genetic testing material post-relationship determination. House Report 116-450 directs that no government agency may use DNA testing results or genetic material for criminal or immigration enforcement.
Revised 08/07/2023; Effective 08/21/2023
5.10.6 Information Sharing for Cases Involving Children Reported Missing
For UCs running away from ORR care or former UCs (“released children”) going missing from sponsor residences, ORR may share information with the National Center for Missing and Exploited Children (NCMEC), a non-profit aiding missing child recovery, child sexual exploitation reduction, and child victimization prevention, enhancing programmed care safety nets. NCMEC collaborates with families, governments, and law enforcement to find missing children and prevent child exploitation.
ORR may also share information with investigative agencies with jurisdiction over missing UC cases:
- Local law enforcement
- State licensing agencies
- Child Protective Services
- Other investigative agencies (HHS Office of Inspector General) with jurisdiction over missing UC cases.
Investigative agencies must submit warrants, investigation numbers, subpoenas, or other documentation to indicate jurisdiction over missing UC cases.
For UC unauthorized absences from ORR care, care providers follow procedures in Section 5.8.1 Emergency Incidents to report to ORR, NCMEC, local law enforcement, and state licensing/CPS (if applicable).
Released children going missing, regardless of PRS referral, may be reported to ORR as missing via the National Call Center. The National Call Center will file Notifications of Concern with investigative agencies (local law enforcement and CPS) for missing released children and report missing released children to NCMEC. If released children are receiving PRS and PRS workers learn of disappearances, PRS providers submit Notifications of Concern per Section 6.8.6 Notifications of Concern. PRS providers will advise sponsors to contact NCMEC. If sponsors do not contact NCMEC, PRS providers will report missing released children to NCMEC.
ORR may provide the following information categories to NCMEC, local law enforcement, or other investigative agencies with missing UC case jurisdiction immediately upon initial missing UC reports or follow-up reports without the case file request process when information sharing is in UC best interests and safety/well-being:
- UC full name and/or alternative spellings and aliases.
- UC A number.
- UC date of birth.
- UC country of birth.
- Recent UC photograph.22
- UC address (ORR care provider facility address or sponsor/post-release address).
- All U.S. family and sponsor contact information.
- All UC country of origin family contact information.
Upon NCMEC request, ORR may also provide telephone and visitor logs from UC time in ORR care during initial or follow-up reports when U.S. and home country family/sponsor contact information is missing/incomplete. Upon local law enforcement or investigative agency requests, ORR may provide telephone/visitor logs from UC ORR care time after UC Bureau Director approval.
In addition to the above, ORR representatives may provide any relevant information assisting NCMEC and/or investigative agencies in missing UC location efforts as part of ongoing consultation and case management. ORR representatives (ORR/FFS, ORR/PO, National Call Center representative, Home Study/Post Release Services (HS/PRS) workers, or care provider staff) may provide summaries of:
- UC descriptive information.
- UC primary language.
- UC endangerments or risk factors (potential trafficking indicators).
- UC online communication history.
- Other circumstantial UC disappearance information.
Case file record requests (case management notes/assessments, clinical notes, trafficking eligibility letters) must be provided to NCMEC, local law enforcement, or other investigative agencies with missing UC case jurisdiction via the case file request process in Section 5.10.1 UC Case File Request Process, requiring warrants, investigation numbers, subpoenas, or other jurisdiction documentation as request support. Mental health and medical case files records must not be provided without appropriate consent as noted in Section 5.9.2 Protecting Confidentiality of Mental Health and Medical Records and only if within investigative agency authority and with UC Bureau Director record sharing consent.
For NCMEC authorization to post UC photos on missing child flyers, appropriate consent must be obtained and documented via the NCMEC Photo Release and Verification form for Social Services Agency Representatives. ORR FFS is authorized to sign NCMEC Photo Release and Verification forms for Social Services Agency Representatives on behalf of ORR for UCs in ORR care. For discharged/released UCs, ORR FFS or ORR Project Officers for PRS providers may sign NCMEC Photo Release and Verification forms for Social Services Agency Representatives on behalf of UC parents/legal guardians if verbal consent is obtained for photo release (documented in UC case files). Sponsors may not sign NCMEC Photo Release and Verification forms for Social Services Agency Representatives on behalf of ORR or UC parents/legal guardians unless they are UC parents or legal guardians. ORR may provide UC photos to other investigative agencies with missing UC case jurisdiction per Section 5.10.1.
If NCMEC or investigative agencies need UC name, family member names, contact information, or other disappearance-related circumstantial information verification after initial missing UC reports, ORR may provide consultation and clarifications as needed to validate information. As noted in Section 5.10.1, ORR is authorized to release documents via the case file request process to NCMEC and other investigative agencies with missing UC case jurisdiction. ORR does not release records to NCMEC, local law enforcement, or other investigative agencies with missing UC case jurisdiction that are outside agency investigation scope or authority without lawful subpoenas or court orders. ORR applies requirements in Section 5.10.1 for document release to NCMEC, local law enforcement, or other investigative agencies with missing UC case jurisdiction under expedited processing without authorizing signatures, and requirements to evaluate record release in UC best interests when UC or caregiver signatures are unobtainable.
In long-term missing UC cases (all leads exhausted, UC not recovered) by NCMEC, local law enforcement, or investigative agencies, agencies may request biometric data as cases progress. For long-term missing UC cases or deceased UCs identified by NCMEC or law enforcement matching missing UC profiles, NCMEC/law enforcement may request UC medical and dental records for deceased UC identification. Under these circumstances, ORR will evaluate requests per Section 5.10.1 requirements and may consent to record release based on UC best interests. Medical/mental health information may only be provided if within investigative agency authority and UC Bureau Director consents to record sharing.
Revised 08/07/2023; Effective 08/21/2023
5.10.7 Information Sharing with Investigative Agencies
ORR shares information with investigative agencies under its policy in Section 5.10 Information Sharing and each agency’s mandate/authority, without releasing information outside investigation scope (see Section 5.10.1.2 Obtaining Authorization from the Subject of the Request. Primary ORR investigative agencies include:
- HHS Office of the Inspector General (HHS/OIG)
- DHS Immigration and Customs Enforcement, Homeland Security Investigations (DHS/ICE/HSI)
- Federal Bureau of Investigation (FBI)
- Government Accountability Office (GAO)
- Local law enforcement
- State Licensing
- Child Protective Services
When additional case file information is requested by investigative agencies beyond information sharing authorized by Sections 5.7.2 Responding to Fraud Attempts, 4.10 Sexual Abuse Reporting and Follow-up, and 5.8 Reporting Child-Level and Program-Level Events, investigative agencies must follow the case file records request process in Section 5.10.1 UC Case File Request Process. Case file record requests are eligible for expedited processing within seven calendar days and should be marked “URGENT” in the subject line (see Section 5.10.1.5 Timeframe for Processing Requests for UC Case File Documents. Case file requests may be further expedited at ORR discretion due to request time-sensitivity.
Mandatory Reporting Requirements
Care providers must report significant incidents to CPS, State licensing, and/or local law enforcement, as appropriate, under mandatory reporting laws, state licensing requirements, federal laws/regulations, and ORR policies/procedures (see Section 5.8 and Section 4.10). Sexual abuse significant incidents must be reported to HHS/OIG and FBI per Section 4.10, and suspected fraud schemes are reported to HHS/OIG per Section 5.7.2 Responding to Fraud Attempts and Section 5.8.2 Significant Incidents. Information may also be provided to investigative agencies with missing UC case jurisdiction per Cases Involving Children Reporting Missing.
Oversight Audits, Evaluations, and Inspections Conducted by HHS OIG and GAO
ORR will comply with turning over case file information (documents, papers, records) outside the case file request process to HHS OIG and GAO when requested as part of UC Bureau oversight audits, evaluations, inspections, or investigations.23 For individual child safety investigations (allegations/complaints affecting <10 children), HHS OIG and GAO (if applicable) must follow case file request processes noted above and in Section 5.10.1 UC Case File Request Process and Section 5.10.6 Information Sharing for Cases Involving Children Reported Missing. ORR will also comply with providing HHS OIG and GAO access to care provider staff and personnel files for interviews/investigations. Case file requests under this section may be further expedited at ORR discretion due to time sensitivity.
Revised 08/07/2023; Effective 08/21/2023
5.11 ORR Child Protection Investigations
UC safety and well-being in ORR care depend on investigations for child abuse/neglect allegations in custody. Typically, state/local authorities conduct these investigations, but in some cases, they will not.
Section 5.11 outlines ORR investigations for child abuse/neglect allegations at certain ORR-funded facilities. These policies implement ORR regulations in 45 C.F.R. Part 412. ORR investigates covered allegations of UC abuse/neglect by covered individuals at (1) care provider facilities in states where state agencies will not investigate allegations at ORR-funded facilities and (2) Emergency or Influx Facilities (EIFs), ensuring consistent programmed care protection standards.
Covered allegations include adult-on-child allegations of child abuse or neglect, such as inappropriate sexual behavior, neglect, medical neglect, physical abuse, sexual abuse, sexual harassment, and verbal or emotional abuse at ORR-funded residential/service facilities for UCs, where state agencies will not investigate such allegations in ORR-funded care provider facilities, and at EIFs.
Covered individuals are care provider facility/EIF staff, contractors/sub-grantees, and volunteers, or other adults with UC access through ORR contracts/grants. Foster parents are not covered individuals subject to ORR investigations, as they remain subject to state licensing requirements and state investigations.
This section details ORR actions in covered allegation investigations, including possible dispositions by the ORR Division of Child Protection Investigations (DCPI).
Five possible dispositions:
- Substantiated at Tier I
- Substantiated at Tier II
- Not substantiated
- Unfounded
- Administratively closed
This section also covers care provider responsibilities during investigations, interventions/staff disciplinary actions, and appeal/review processes for Tier I/Tier II substantiated perpetrators, ensuring accountability within programmed care.
Effective 01/10/2025
5.11.1 Investigations of Allegations of Child Abuse or Neglect
Care providers must report Child-Level Events (CLEs) regarding child abuse/neglect allegations to ORR per Policy Guide Section 5.8 Reporting Child-Level Events and Program-Level Events. ORR Prevention of Child Abuse and Neglect (PCAN) staff receive and review these CLEs, ensuring vigilant programmed care oversight.
Child abuse and neglect mean any act or failure to act resulting in death, serious physical/emotional harm, sexual abuse, or UC exploitation; or imminent serious harm risk, including physical abuse, verbal/emotional abuse, sexual harassment, sexual abuse, inappropriate sexual behavior, neglect, and medical neglect.
Within 24 hours of report receipt, PCAN will refer allegation types meeting this definition (“covered allegations”) to DCPI for evaluation when incidents occur in states not investigating UCs in ORR custody or at EIFs.
Upon receiving reports, DCPI will first evaluate to confirm that child abuse/neglect allegations meet adult-to-child abuse/neglect criteria as defined in the Guide to Terms when initially receiving Significant Incident Reports (SIRs) for covered allegations. During intake, DCPI will review reports to assess risk of harm (potentially harmful conditions/situations, not necessarily immediate/severe) or substantial risk of harm (conditions/behaviors likely to result in serious harm if unaddressed). DCPI will determine if allegations require immediate response based on alleged victim risk levels, assign different response times, and designate one of the following actions:
| INTAKE DETERMINATION TYPE | INTAKE DETERMINATION TYPE DESCRIPTION |
|---|---|
| Assigned for Investigation | DCPI Supervisor assigns an ORR DCPI Child Welfare Investigator to investigate child abuse/neglect reports, and the subject of investigation is categorized as an “alleged perpetrator”. |
| Administratively Closed | Intake reports are administratively closed when DCPI determines it will not seek to make a disposition of covered child abuse/neglect allegations. |
Administrative closure can occur at any point. If reports are administratively closed and not assigned for investigation at intake, closure notifications will be provided to reporters and/or care provider facilities. DCPI may administratively close reports at intake in circumstances including:
- Lack of jurisdiction to investigate allegations (alleged abuse/neglect in states where state agencies investigate reports in ORR care).
- Report transfer to another jurisdiction/agency.
- Covered allegations not meeting abuse/neglect definitions.
- Inability to locate alleged UC victim.
- Already investigated covered allegations.
- DCPI intake report duplication.
- Exigent circumstances/conditions making investigation impossible.
Investigations will be initiated immediately, within 24 hours, 72 hours, or 10 calendar days based on evaluated UC risk levels, ensuring timely programmed care responses.
During investigations, DCPI will at minimum:
- Immediately request potential video/documentary evidence preservation.
- Establish a thorough investigation plan.
- Review care provider facility records (intake reports) on alleged victims and perpetrators.
- Conduct updated background checks on alleged perpetrators, including FBI fingerprint checks of national/state criminal history repositories, National Sex Offender Public Website checks, state child abuse/neglect registry checks, and other public records checks.
- Interview allegation reporters (if not interviewed during intake).
- Review evidence of past conduct resulting in Tier II substantiated and not substantiated dispositions related to the same alleged perpetrator (if applicable).
DCPI may form multidisciplinary teams of ORR staff and subject matter experts to review case facts with assigned ORR Child Welfare Investigators, as needed.
In addition to investigating covered allegations, DCPI will also evaluate imminent/ongoing child abuse/neglect risks to UCs remaining in care provider facilities. If risks/concerns are identified, DCPI will require safety plan implementation during investigations and may collaborate with Contracting Officer’s Representatives (CORs) or Project Officers (POs) to ensure ongoing risk mitigation and UC safety plans.
When investigations begin, alleged perpetrators will be added to an internal ORR pending registry to prevent hiring at ORR-funded facilities during DCPI investigations. If other authorities also investigate the same covered allegations (local, state, federal agencies, law enforcement), DCPI will coordinate to avoid investigation disruption/interference. DCPI will provide written Notifications of Investigation to inform relevant parties upon investigation initiation, ensuring transparent programmed care processes. Provided UCs (14+) consent, DCPI will also notify alleged victim parents, legal guardians, or sponsors. For alleged victims under 14 or with developmental disabilities, ORR will determine in its discretion and considering UC best interests whether to notify parents, legal guardians, or sponsors. Relevant parties include:
- Alleged victim.
- Care provider of alleged victim UC at the time of the incident.
- Alleged victim parents/legal guardians.
- Alleged perpetrator.
- Alleged victim attorney of record (if any).
- UC current sponsor (if applicable).
DCPI will conclude investigations after ORR Child Welfare Investigators have made every effort to determine findings within 60 calendar days of case assignment. Investigations may be paused/resumed in 30-day increments with DCPI Supervisor or Director approval.
Following investigation completion, DCPI will issue dispositions for each reported allegation under investigation, based on a preponderance of evidence (evidence showing abuse/neglect more likely than not). This standard guides DCPI in determining case dispositions:
- Substantiated Tier II: Preponderance of evidence establishes abuse/neglect, but aggravating/mitigating factors do not warrant Tier I findings.
- Not Substantiated: No preponderance of evidence establishing abuse/neglect, but evidence indicates UC harm or risk.
- Unfounded: No preponderance of evidence establishing abuse/neglect, and evidence indicates UC was not harmed or at risk.
- Administrative Closure: DCPI determines it will not seek to make a disposition for covered abuse/neglect allegations.
Within five calendar days of disposition, DCPI will notify alleged perpetrators via certified mail. Within five calendar days of disposition, DCPI will provide written Notifications of Disposition to care providers (EIFs), alleged victims, and alleged victim attorneys of record (if any). Provided UCs (14+) consent, DCPI will notify parents, legal guardians, or sponsors with written notifications. For alleged victims under 14 or with developmental disabilities, ORR will determine in its discretion and considering UC best interests whether to notify parents, legal guardians, or sponsors.
If abuse/neglect allegations are not substantiated, unfounded, or administratively closed, dispositions will be issued with no further action.
If DCPI substantiates abuse/neglect allegations, alleged perpetrators will be categorized as substantiated perpetrators at Tier I or Tier II. Notifications of Disposition for substantiated perpetrators will summarize DCPI substantiation bases. Notifications of Disposition will inform substantiated perpetrators of Administrative Law Judge (ALJ) appeal requests to the HHS Departmental Appeal Board (DAB) and include appeal initiation steps (see Section 5.11.4 HHS Departmental Appeals Board and ACF Assistant Secretary Appeals and Review Process). Notifications of Disposition will also inform substantiated perpetrators that failure to submit written appeal requests within 30 calendar days of Notice of Disposition receipt will waive appeal rights (referenced in Section 5.11.3 Interventions and Discipline) and subject them to:
- Tier I substantiated perpetrators being referred to the ORR Central Registry (ORR database of Tier I substantiated child abuse/neglect perpetrators after the 30-day appeal request timeframe). This registry is separate from the internal registry tracking alleged perpetrators during active investigations. Registry listing prohibits working/volunteering on ORR-funded grants/contracts and UC access in ORR custody or the UC Portal.
- Tier II substantiated perpetrators being maintained in ORR records as Tier II sustained perpetrators.
Effective 01/10/2025
5.11.2 Obligations of Care Provider Facilities (including Emergency or Influx Facilities)
Care provider facilities (including EIFs) must take immediate action upon awareness of covered allegations involving UC abuse/neglect, ensuring UC safety and compliance with investigative procedures, reinforcing programmed care safety protocols. ORR Central Registry checks must be conducted for all staff at least annually, coordinated with ORR Project Officers (POs).
Required Responsive Actions:
Care providers (including EIFs) must take the following steps when covered allegations are reported to minimize potential UC risk while investigations are ongoing:
Access to Supports for Unaccompanied Children
Care providers must ensure the following UC supports and services:
- Legal Representation and Family Access:
- UCs must have access to attorneys of record (if any) or other legal service providers (LSPs).
- UCs must have family access (including legal guardians), unless ORR has documented safety reasons prohibiting access.
- Embassy or Consulate Access:
Provide UCs with opportunities to contact their consulates/embassies for support. UCs with immigration case concerns are encouraged to consult attorneys of record/LSPs before contacting consulates/embassies.
Note: While UCs with credible fear/asylum claims must be afforded this opportunity, care providers are not required to proactively share UC claims with consulates/embassies. Requirements like death notifications remain mandatory (see Policy Guide Section 3.3.16 Notification and Reporting of the Death of an Unaccompanied Child).
Implementation of a Safety Plan:
Care providers must implement comprehensive safety plans when responding to covered allegations, tailored to individual UC needs and addressing immediate safety concerns, ensuring responsive programmed care.
- Comprehensive Safety Plan Development: Safety plans must be developed for UC physical/emotional well-being, outlining specific steps, services, and resources, such as medical care, crisis intervention, counseling, or support systems. Plans must be responsive to immediate UC needs during/after investigations as outlined in Section 3.3.4 Safety Planning. UC needs may inform release decisions, but ORR does not delay release unless consistent with Section 2.7.4 Deny Release Request or other ORR requirements.
- Collaboration with DCPI and ORR: DCPI may collaborate with care provider POs/FFSs and elevate concerns requiring Corrective Action Plans or additional monitoring to address identified concerns. Care providers must immediately address DCPI, PO, or FFS-identified concerns, ensuring proactive programmed care management.
Monitoring and Enforcement:
ORR may take monitoring/enforcement actions when care provider facilities interfere with, delay, or fail to permit investigations, ensuring accountability in programmed care. These actions include:
- Remote or on-site monitoring.
- Corporate office monitoring for internal policies, reporting structures, and supervisory responses.
- Limiting or stopping new UC placements.
- Removing all UCs from facilities and placing them in other facilities.
- Issuing corrective actions.
- Terminating cooperative agreements/contracts.
- Imposing remedies for HHS grant recipient/contractor non-compliance (e.g., 45 C.F.R. §75.371 remedies).
ORR also requires immediate suspension with pay of alleged perpetrators suspected of sexual abuse/harassment from all duties involving UC contact/access pending investigation outcomes (see UC Policy Guide Section 4.3.5 Staff Code of Conduct). Alleged perpetrators must remain suspended throughout investigations until case dispositions. Care providers must obtain COR/PO approval before lifting suspensions/reassignments of alleged perpetrators with not substantiated or unfounded dispositions. Alleged perpetrators with Not Substantiated, Unfounded, or Administratively Closed dispositions may be removed from suspension/reassignment.
Care providers (including EIFs) where DCPI investigates covered allegations may take disciplinary measures where covered individuals exhibit behavior not rising to substantiated allegation Tier I levels but raising child welfare concerns. This includes retaliation against good-faith reporters/investigation participants. Incidents of this nature should also be reported as referenced in 4.3.5 Staff Code of Conduct, 4.10.1 Methods for Children and Youth to Report, and 4.10.2 Care Provider Reporting Requirements. Care providers must also address employee misconduct via internal review consistent with employee conduct policies/procedures, including return-to-work decisions. Post-final case disposition, care providers must create SIR addendums per Section 5.8.4 Report Addendums.
Care providers (including EIFs) must notify attorneys of record, LSPs, child advocates, parents/legal guardians, and potential sponsors of investigations resulting from Significant Incident Reports (SIRs) requiring stakeholder notification as appropriate (see Section 4.10.4 Notification and Access to Attorneys/Legal Representatives, Families, Child Advocates, and Sponsors and Section 5.8.11 Notification to Attorneys, Legal Representatives, Child Advocates, Families, and Sponsors).
ORR requires care providers (including EIFs) to fully cooperate with DCPI during covered child abuse/neglect allegation investigations. Care providers are prohibited from internal investigations of abuse/neglect allegations actively under DCPI investigation, ensuring unbiased programmed care oversight. During DCPI investigations, care providers (including EIFs) must:
- Temporarily reassign alleged perpetrators to duties without direct UC contact/UC Portal access, minimizing UC risk.
- Immediately notify alleged perpetrators of DCPI investigations, as appropriate. If safety concerns for staff, alleged victims, or other children exist, notification may be delayed to take facility safety measures. Care providers must not share information compromising DCPI/concurrent criminal investigations with alleged perpetrators but can share updates on investigation initiation, case disposition, and employment status/task assignments.
- Provide UCs access to health services (specialists, mental health practitioners), individual counseling, and crisis intervention for appropriate UC needs response, ensuring comprehensive programmed care. For sexual abuse/harassment investigations, UCs must be offered community service provider access (see Section 4.5 Responsive Planning).
- Provide UCs access to attorneys of record/LSPs, families (including legal guardians), unless ORR has documented safety reasons prohibiting access.
- Alleged sexual abuse/harassment victims must be provided consulate/embassy contact opportunities.
- Permit DCPI unrestricted access to premises, physical property, buildings, staff, and UCs in facility custody.
- Implement DCPI-directed safety plans to mitigate child abuse/neglect risks and ensure UC safety at facilities for concerns requiring immediate response. DCPI may collaborate with care provider POs/FFSs and elevate concerns requiring Corrective Action Plans or additional monitoring to address identified concerns.
- Permit DCPI to conduct interviews with UCs at facilities without care provider facility staff, contractors, sub-recipients, or volunteers present.
- Within legal privacy rights limits, permit DCPI to observe care provider facility staff, contractors, sub-recipients, volunteers, or other individuals with UC access via ORR contracts/grants activities.
- Promptly preserve potential video/documentary evidence and, within legal privacy rights limits, promptly provide access to all requested files, records, reports, data, and video recordings to DCPI within one business day of request receipt.
- Promptly submit complete and accurate written question responses within one business day.
- Fully cooperate with other state, local, and federal entity/agency and law enforcement investigations of covered allegations. Investigative agencies must follow the case file records request process in Section 5.10.1 UC Case File Request Process.
ORR may take monitoring/enforcement actions when care provider facilities interfere with, delay, or fail to permit investigations, including desktop/on-site monitoring, corporate office monitoring, limiting/stopping UC placements, removing all UCs, corrective actions, facility closure, or remedies for HHS grant recipient/contractor non-compliance (45 C.F.R. §75.371 or similar regulations), ensuring accountability in programmed care oversight.
Revised 1/10/2025
5.11.3 Interventions and Discipline
ORR requires specific interventions and discipline for DCPI-substantiated covered allegations, ensuring consistent programmed care accountability. These include ORR and care provider facility measures.
If Tier II substantiated perpetrators waive appeal/review opportunities or DCPI dispositions are upheld post-appeal/review (see Section 5.11.4 HHS Departmental Appeals Board Appeals and ACF Assistant Secretary Review Process), individual information will only be recorded/maintained in agency records as Tier II sustained perpetrators, separate from the ORR Central Registry. Tier II sustained perpetrators will not face additional ORR disciplinary action for specific allegations. However, ORR may use their records to identify abuse/neglect patterns and guide future facility safety planning, informing proactive programmed care strategies.
If Tier I substantiated perpetrators waive appeal/review opportunities or DCPI dispositions are upheld post-appeal/review, substantiated perpetrators will be subject to:
- Referral to the ORR Central Registry:
- Tier I substantiated perpetrators will be listed in the ORR Central Registry as Tier I sustained perpetrators, containing names, identifying information, and underlying child abuse/neglect allegation details. The Registry only applies to DCPI-investigated individuals, not state/local substantiated findings.
- The ORR Central Registry is not publicly available. Listed individuals may be referred to relevant state/local entities and law enforcement agencies in the state of abuse/neglect by DCPI Registry per 45 C.F.R. §412.101(d)(1). Out-of-state agency information requests will be reviewed case-by-case.
- ORR will use the ORR Central Registry to identify Tier I Sustained Perpetrators as part of care provider facility screening processes described in Section 4.3.3.1 ORR Required Background Investigations. ORR Central Registry-listed individuals are prohibited from working/volunteering on ORR-funded grants/contracts and UC contact in ORR custody or UC Portal access.
Five years after initial Central Registry entry and with no further substantiated abuse/neglect allegations, Tier I substantiated perpetrators may submit written requests to DCPI at [email protected] for name removal. ORR will review requests case-by-case. For sexual penetration, child death, sexual molestation, or sexual exploitation cases, records will be maintained for 25 years. Unfounded allegation records are maintained and disposed of per federal records management requirements, ensuring compliant programmed care data management.
- Employment Prohibition:
- ORR Central Registry-listed individuals are prohibited from working/volunteering on ORR-funded grants/contracts and UC contact in ORR custody or UC Portal access, unless ORR removes them from the registry.
- As part of care provider facility staff, contractor, sub-grantee hiring screening, or care provider facility volunteer allowance, all care provider facilities, regardless of state child abuse/neglect investigation status, must confirm with ORR Project Officers/Contract Officer’s Representatives (CORs) that applicants are not on the ORR Central Registry.
- All care provider facilities, regardless of state investigation status, must annually check all personnel against the ORR Central Registry, ensuring proactive programmed care staff safety measures.
- Disciplinary Sanctions:
- Care provider facilities must take appropriate remedial measures when staff, contractors, or volunteers exhibit behavior not meeting child abuse/neglect definitions but violating staff codes of conduct (see Section 4.3.5 Staff Code of Conduct) or raising child welfare concerns (retaliation, investigation interference).
- DCPI-directed remedial measures may prohibit relevant care provider facility staff, contractor, or volunteer UC contact.
- Referrals to State, Local, and Other Federal Agencies
- ORR will refer substantiated perpetrator names to relevant state/local entities and law enforcement agencies in the state of abuse/neglect. If state/local authorities or relevant law enforcement agencies outside the state of sustained Tier I allegations request information about sustained perpetrators, ORR will confirm if individuals are on the ORR Central Registry per 45 C.F.R. §412.101(d)(1) before information release, ensuring responsible programmed care information sharing.
- ORR will refer Tier I sustained perpetrator names to the FBI and HHS Office of the Inspector General (OIG) consistent with applicable agreements.
- ORR and care provider facilities shall not interfere with other state, local, or federal entity/agency investigations of child abuse/neglect.
Investigation findings may assist in completing U and T visa certifications, supporting UC legal relief within programmed care. Care providers should ensure UC access to LSPs/attorneys of record for consultation, as findings may impact immigration cases. U/T visa certification requests should be emailed to DCPI at [email protected].
Effective 1/10/2025
5.11.4 HHS Departmental Appeals Board Appeals and ACF Assistant Secretary Appellate Review Process
The ORR Unaccompanied Children Bureau (UCB) and HHS Departmental Appeals Board (DAB) have established two separate optional procedures, at personal cost to substantiated perpetrators, following Notification of Disposition receipt, ensuring due process within programmed care:
- Appeal Process: Substantiated perpetrators may appeal ORR substantiated dispositions to an Administrative Law Judge (ALJ) at the HHS Departmental Appeals Board (DAB).
- If substantiated perpetrators submit appeal notices not dismissed by ALJs, ORR must notify alleged victims, victim attorneys of record (if any), and, as appropriate and determined by ORR, alleged victim parents, legal guardians, or sponsors (absent non-consent of children 14+) that ALJ appeals will be conducted. Alleged victims, witnesses, and family members will not be required to testify, minimizing UC burden within programmed care.
- Substantiated perpetrators may choose appeal via telecommunications technology or documentary submission.
- Failure to submit appeal requests within 30 calendar days will be deemed a waiver of appeal rights, and appeals will be dismissed.
Dismissal of Appeal Requests
ALJs will dismiss appeal requests under the following circumstances:
- Requests are not received within 30 calendar days of substantiated perpetrator Notification of Disposition receipt.
- Failure to demonstrate good cause for untimely requests (ALJ determination).
- Request withdrawal or abandonment (no communication for 30 days).
Individuals filing appeals of “not substantiated,” “unfounded,” or “administratively closed” dispositions (ineligible for appeal) will have requests dismissed. If appeals are initially dismissed, DAB may, at its discretion, temporarily remove Tier I or Tier II sustained perpetrator designations (temporary removal from ORR Central Registry for Tier I and ORR agency records for Tier II). This action may be granted when DAB ALJs determine individuals have established good cause for missing original appeal deadlines, allowing for appeal rescheduling and subsequent ALJ final decisions if perpetrators re-establish communication, ensuring fair process within programmed care.
Disclosure of Case Materials
Upon timely appeal requests, ORR will provide substantiated perpetrators and legal counsel with all disposition information except portions that:
- Compromise UC, reporter, or other person safety/well-being.
- Reveal identities of UCs providing information with confidentiality understandings.
- Reveal identities of alleged perpetrators with unfounded dispositions in the same case.
- Are otherwise prohibited by state/federal law.
Outcome of Appeal
- If Tier I perpetrators waive appeal rights or ALJs uphold dispositions, individuals will be added to the ORR Central Registry as Tier I sustained perpetrators.
- For Tier II perpetrators, if appeal rights are waived or ALJs uphold dispositions, ORR will not impose further disciplinary action. However, records may still be reviewed for abuse/neglect pattern identification and future safety planning, informing continuous programmed care improvement.
- Cases may be remanded to DCPI if ALJs determine evidentiary records are insufficiently complete to decide if ORR dispositions are supported by a preponderance of evidence.
Notification and Appeal Determination
- If appeal requests are granted and appeals proceed, ORR must notify alleged victims, victim attorneys of record (if any), and, as appropriate and determined by ORR, alleged victim parents, legal guardians, or sponsors (absent non-consent of children 14+) that appeals will be conducted. Alleged victims, witnesses, and family members will not be required to testify, minimizing UC burden within programmed care.
- ALJ written decisions to uphold, modify, or reverse DCPI dispositions will be served to relevant parties, including the Assistant Secretary for Children and Families, alleged victims, victim attorneys of record (if any), and, as appropriate and determined by ORR, alleged victim parents, legal guardians, or sponsors (absent non-consent of children 14+).
- ALJ final decision notifications will include instructions for requesting Assistant Secretary for ACF review.
- Review by the Assistant Secretary for Children and Families
Tier I or Tier II substantiated perpetrators may request Assistant Secretary for Children and Families review of ALJ decisions within 30 calendar days of receipt.
- Within 30 days of timely requests, Assistant Secretaries for ACF may affirm, modify, or reverse ALJ decisions, including cases dismissed for untimeliness or procedural defects. Reviews will assess if ALJ decisions were based on significant legal/factual errors.
- If Assistant Secretaries affirm ALJ decisions, or no modifications are made within 30 calendar days of request receipt, ALJ decisions become final and binding on all parties, ensuring definitive outcomes in programmed care accountability processes.
- If no review requests are made, Assistant Secretaries have an additional 30 calendar days to review decisions at their discretion. If no changes are made, ALJ decisions become final, and substantiated perpetrators will be considered Tier I or Tier II sustained perpetrators (see UC Policy Guide Section 5.11.3 Interventions and Discipline).
Final Decision and Notifications
- If Tier I perpetrators waive review rights or Assistant Secretaries uphold dispositions, individuals will be added to the ORR Central Registry as Tier I sustained perpetrators.
- For Tier II perpetrators, if review rights are waived or Assistant Secretaries uphold dispositions, ORR will not impose further disciplinary action. However, records may still be reviewed for abuse/neglect pattern identification and future safety/investigations prompted by new allegations, informing continuous programmed care improvement.
- The Office of the Assistant Secretary will serve copies of final decisions to all involved parties, including alleged victims, victim attorneys of record (if any), and, as appropriate and determined by ORR, alleged victim parents, legal guardians, or sponsors (absent non-consent of children 14+).
Effective 1/10/2025
Footnotes
1. Emergency Supplemental Appropriations for Humanitarian Assistance and Security at the Southern Border Act, 2019, Pub. L. 116-26
2. At this time the Central American countries of El Salvador, Guatemala and Honduras are not mandatory notification countries. Mexico is not a mandatory notification country, but the U.S. does have a bilateral agreement that confers similar protocols for children, therefore Mexican consulate officials will be given access to unaccompanied children under similar arrangements as a mandatory notification country.
3. If there has been a court ordered termination of parental rights, a fear that the child is a victim of abuse or trafficking, or that contacting the parent or legal guardian would place the unaccompanied child in danger, the care provider will contact the consulate without the parent/legal guardian’s permission (unless the child is claiming credible fear or asylum). If the care provider is unsure, they should immediately elevate their concerns to the ORR/FFS assigned to the care provider.
4. See Exhibit 1, para. C of the Flores settlement agreement.
5. For report templates, see https://www.grants.gov/forms/forms-repository/post-award-reporting-forms
6. The ORR Case Management database has a firewall in place to prevent access outside the United States and its territories.
7. Sponsors may be required to pay for the transport of a child (and the travel of any escorts). See Section 2.8.2 Transfer of Physical Custody
8. For Program-Level Events (PLE) reporting purposes, an outbreak is defined as four (4) or more cases of an infectious disease (e.g., influenza, norovirus, strep throat) within a two (2) week period. Individual cases of notifiable diseases are reportable to ORR through other mechanisms. Care providers must also be aware of notifiable disease and outbreak reporting requirements in their States, as outlined in Section 3.4.6 Management of Communicable Diseases.
9. Unaccompanied Children’s case files and program records should be maintained and shared in adherence to what is set out in the System of Records Notice for the Unaccompanied Children’s program 81 FR 46682, or any updated Systems of Records Notice as is published for the Unaccompanied Children’s Bureau.
10. As a matter of discretion ORR treats information maintained in ORR system of records on non-U.S. persons, including case files containing information about children and sponsors, as being subject to the provisions of the Privacy Act. Office of Management and Budget (OMB) guidance allowing agencies discretion to treat mixed systems as subject to the Privacy Act, OMB Privacy Act Implementation: Guidelines and Responsibilities, 40 Fed. Reg. 28948 (PDF)(PDF), 28951 (July 9, 1975). Specifically, the 1975 OMB guidance states: Files relating solely to nonresident aliens are not covered by any portion of the [Privacy] Act. Where a system or records covers both citizens and nonresident aliens, only that portion which relates to citizens or aliens is subject to the Act, but agencies are encouraged to treat such systems as if they were, in their entirety, subject to the Act.
11. The Joint Explanatory Statement on Consolidated Appropriations, 2021-Division H (PDF)(PDF) directs ORR to develop specific policies and procedures regarding the confidentiality of counseling and mental health services provided to unaccompanied children, as well as all related documentation, consistent with applicable child welfare laws and regulations, and to ensure care providers are informed of such policies.
12. The House Report 116-450 (PDF) directs ORR to refrain from sharing mental health information with immigration court for master calendar hearings where the court is not making decisions about a child’s custody. The House Report 116-450 (PDF) further restricts ORR from sharing mental health records with EOIR unless ORR or the care provider is appearing as party in a legal proceeding.
13. ORR tries to provide for the veracity of who the parent or legal guardian is based on its records.
14. Diagnosed developmental disability in this context refers to a diagnosed condition that impacts the child’s cognitive capacity to consent. Examples of this would include, but are not limited to an intellectual disorder, neurocognitive disorder, or severe psychiatric disorder. The assessment of whether a child can consent to release of records must be determined by a physician, nurse practitioner, psychologist, or psychiatrist, following a diagnosis of a cognitive disorder that impacts capacity to consent. Diagnosis of a disability alone is not sufficient to determine whether a child has the capacity to consent for release of their information. If ORR reasonably believes there is a competency concern, while pending the diagnosis or assessment, ORR could make a best interests determination on behalf of the child.
15. ORR refers children who are child trafficking victims and other vulnerable children to be appointed a Child Advocate (see 8 U.S.C. 1232(c)(6)). Under the authorities of the Trafficking Victims Protection Reauthorization Act of 2008 (TVPRA) (PDF), ORR refers children who have a developmental disability, tender age children, children who are pregnant or parenting, children who are placed in a restrictive or therapeutic setting, children who are within six (6) months of aging out where family reunification is unlikely, and children who have been a victim of a crime or human trafficking to be appointed a Child Advocate.
16. If the records request is from a government agency (federal, state, or local), ORR will notify a child’s attorney of record or Child Advocate if assigned of the records request to provide notice of the request. The child’s attorney of record and Child Advocate will be given an option to notify ORR within two (2) business days of receipt if there is any objection to the release of this information.
17. In general, a “lawfully-issued” subpoena is a subpoena was that was issued in accordance with applicable law. ORR staff and care providers should consult with their general counsel to determine if a subpoena was lawfully-issued.
18. Note that a copy of this form must be provided to the child’s LSP or attorney of record, and Child Advocate after provision to EOIR.
19. For children under the age of 14 or children with a diagnosed developmental disability, the care provider should ask the child’s parents for their consent for their contact information to be shared with the LSP.
20. ORR notifies the LSP whenever ORR finds out there is a removal order pursuant to MPP, whether before or after the KYR and legal screening are conducted. ORR also notifies the LSP before transfer of the child with an MPP removal order to another care provider facility.
21. In general, this policy describes information sharing policies regarding children in ORR care who were separated from parents/legal guardians by DHS at the southern border, as described in Ms. L. v. U.S Immigr. & Customs Enf’t (“ICE”), 310 F. Supp. 3d 1133 (S.D. Cal. 2018), modified, 330 F.R.D. 284 (S.D. Cal. 2019), and enforcement granted in part, denied in part sub nom. Ms. L. v. U.S. Immigr. & Customs Enf’t (“ICE”), 415 F. Supp. 3d 980 (S.D. Cal. 2020). Where the circumstances of separated children in ORR care differ from those described by the Ms. L. litigation, or by other legal requirements (e.g., House Report 116-450), this sub-section may not apply.
22. The child’s photograph may not be shared with DHS or EOIR absent one of the covered exceptions outlined in Section 5.10.2 Limits to Sharing Information with DHS and EOIR.
23. ORR will provide records to OIG and GAO in compliance with 45 CFR § 75.364 Access to records.